Background:
Medical students and interns often lack formal training on how to initiate a consult, resulting in a potentially unpleasant experience for both parties. Most current literature addressing consult etiquette involves either outpatient referrals or are directed to consultant services. Our goal was to describe inpatient consult initiation and etiquette by internal medicine teams at a single academic medical center.
Methods:
We performed a qualitative study to explore inpatient consult etiquette, defined as how the primary medical team prepares for a consult, contacts, and communicates with a medical specialty consultant. We held focus groups and one-on-one interviews of fourth year medical students, interns, and hospitalists, as well as internal medicine subspecialty fellows and faculty. A standardized discussion template was used to explore consulting behaviors, consequences of poor etiquette, and barriers to proper etiquette. Data was collected until thematic saturation was reached. The interviews were transcribed and content analysis was performed. This involved two reviewers independently coding the data to determine common themes.
Results:
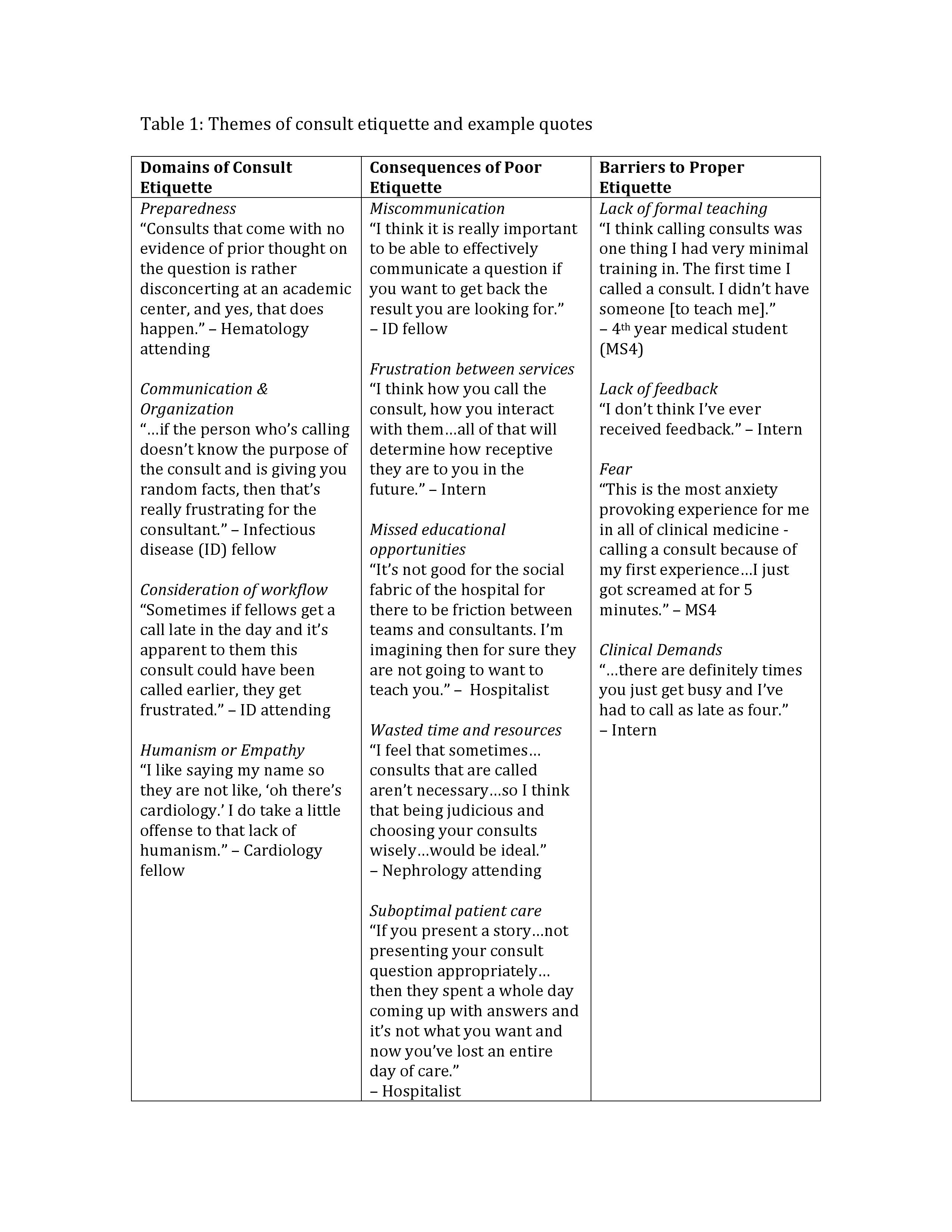
We performed 2 focus groups and 8 interviews consisting of 13 primary medical team providers and 8 consultants, many with training from different academic institutions. Consultants mentioned that common areas of improvement were in the preparation and initial management of the patient, organization of communication, consideration of workflow, and humanism in a professional environment. Both medical team providers and consultants noted that poor consult etiquette leads to miscommunication of goals, frustration between services, missed educational opportunities, and wasted time and resources, all of which could lead to suboptimal patient care. Most medical providers and consultants noted receiving little direction or feedback when they started calling consults, which often led to fear or anxiety from negative consultant responses. Table 1 lists these themes and associated quotes generated by both groups.
Conclusions:
We identified several key domains of inpatient consult etiquette and found that improper consult etiquette is perceived to negatively affect patient care and relationships between services. Our findings will allow us to develop a formal curriculum to improve communication between primary medical teams and consultants in a teaching hospital setting.