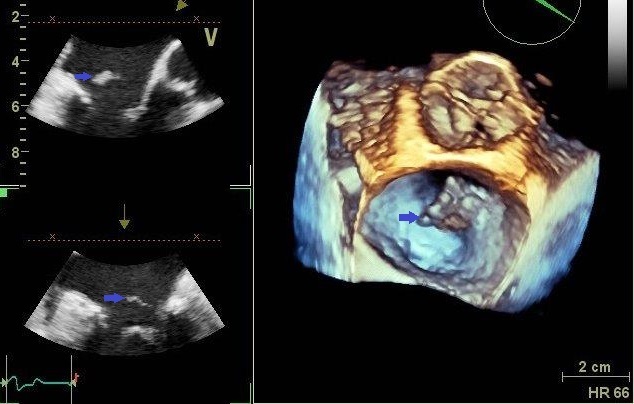
Case Presentation: A 59-year-old female with history of well-controlled type 2 diabetes mellitus and hypertension presented with one-week history of high-grade fever (Temp 101 F), nausea, generalized weakness, and postural hypotension. She denied any diarrhea, chest pain, loss of consciousness, tinnitus, or visual changes. Patient also refuted any prior history of intravenous drug abuse. Physical examination was remarkable for sinus bradycardia with heart rate of 42 bpm, and a right hallux wound. Laboratory analysis was significant for leukocytosis (14.6 x 109/L with neutrophilia) and troponin of 0.048 ng/mL. Electrocardiogram revealed a new third degree heart block. Emergent trans-venous pacemaker was placed. Blood cultures drawn at the time of admission grew Corynebacterium striatum (C. striatum) in two out of four bottles, which was disregarded as a contaminant. Transthoracic echocardiogram (TTE) was done to preclude ischemia as the cause of heart block. Patient was found to have a mitral valve vegetation on TTE. Vancomycin was started for management of infective endocarditis. Subsequent trans-esophageal echocardiogram confirmed mitral valve vegetation measuring 2.4 x 1.5cm with possible extension to the posterior interatrial septum. She underwent removal of mitral valve vegetation, debridement of cardiac abscess, and mitral valve repair. Cultures from valve vegetation also grew C. striatum. Patient was treated with vancomycin for a total of 6 weeks with complete resolution of infection.
Discussion: The epidemiological profile of infective endocarditis has been changing over the past decade. Infective endocarditis due to Corynebacterium striatum (a gram-positive rod of the diphteroid species) is uncommon, and is associated with underlying valve disease, prosthetic valves, intra-cardiac devices, immunosuppression, presence of indwelling catheters, intravenous lines, and hemodialysis. As per literature search, there have been a few case reports of C. striatum endocarditis in immunocompetent patients with recent hospital admission and intravenous line placement. To our knowledge, this is the first reported case of diphtheroid infective endocarditis involving a normal native valve in an immunocompetent patient with no risk factor(s) present. We believe that the foot ulcer was the route of entry of the bacteria to her blood stream.
Conclusions: C. striatum is a skin commensal organism which is considered a contaminant in most blood cultures. In the hospital setting, positive blood cultures for C. striatum should never be overlooked. More research is warranted to document the pathogenicity of this organism.