Background: Outpatient management of UTI as a treatment option was firmly established by Hoberman’s study in 1999 and confirmed in Cochrane reviews in 2003 and 2007 yet admission rates remained constant through 2009. In 2011 the AAP UTI guidelines were revised, again reinforcing the outpatient option. Our objective was to see if the 2012 Kids’ Inpatient Database (KID) data would reflect any decrease in UTI discharges
Methods: We examined KID, a national dataset available through AHRQ, from 1997-2012, through HCUPnet. KID data is triennial. Discharge volume for CCS principal diagnosis category 159 Urinary tract infection was examined for trends across years by age (as grouped by KID). Changes in length of stay (LOS) and charges corrected for inflation (using http://data.bls.gov/cgi-bin/cpicalc.pl) were also examined.
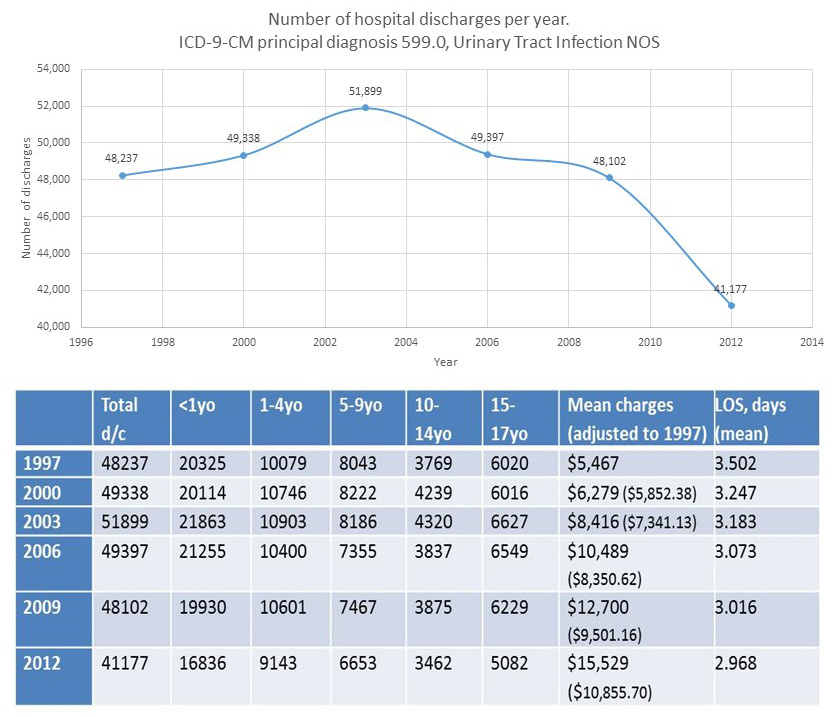
Results: There were significantly fewer UTI discharges in 2012 than 1997-2009 (p .001).The largest decrease was in <1yo and 1-4 yo. LOS has trended down consistently and charges have increased to almost double corrected for CPI.
Conclusions: 2012 represents the first significant decrease in total national discharge for UTI since KID started in 1997. This coincides with the 2011 AAP UTI guideline revision as the culmination of evidence for more outpatient management over the preceding decade. The largest age group decrease was <1yo then 1-4yo, overlapping the AAP guideline population of 2-24 months. Further study needs to be done to explain causes of substantially increased and continuously rising charges for a disease for which treatment has not been dramatically altered over the study period.