Case Presentation: A 40 year-old male with no significant past medical history presented with two months of increasing fatigue, anorexia, and progressive exertional dyspnea. Additionally, he reported a mild increase in abdominal girth during the same time span. On the day of admission, the patient experienced nausea, vomiting, and severe dyspnea while playing soccer and presented to the emergency department. On review of systems, he denied any headaches, palpitations, or episodes of sweating.
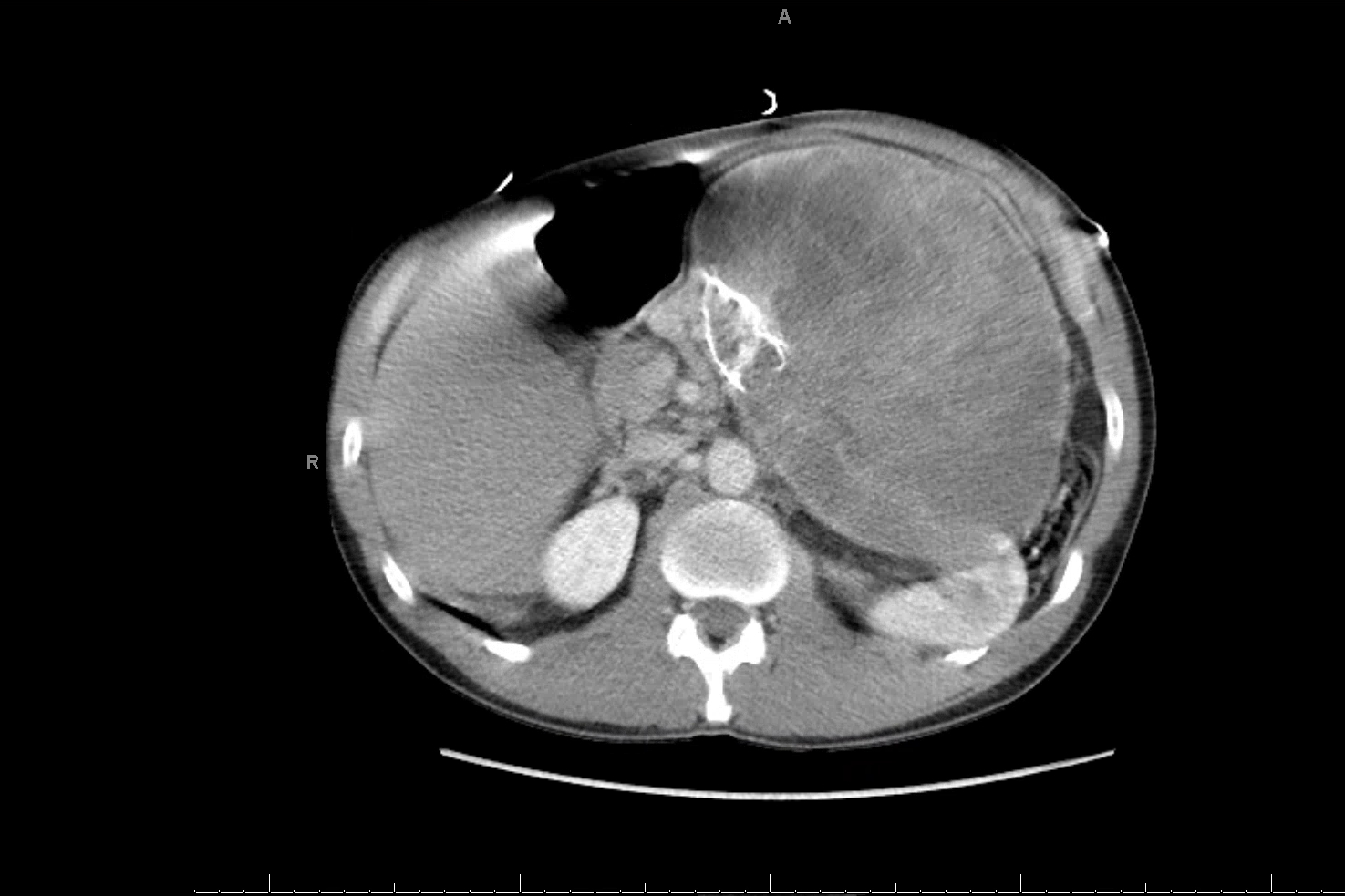
On arrival, the patient was tachycardic, hypertensive, dyspneic and hypoxic. His exam was significant for diffuse inspiratory crackles and a palpable large and tender left sided abdominal mass. CT of the chest, abdomen, and pelvis revealed pulmonary edema and a large retroperitoneal mass, measuring 21 cm x 20 cm x 13 cm with cystic, solid, and calcified components (Figure 1). The mass appeared independent of his kidneys, adrenals, pancreas or spleen. His initial blood work was significant for an elevated troponin level. An echocardiogram showed an ejection fraction of less than 20% with global hypokinesis and segmental wall motion abnormalities.
The patient was treated for heart failure with aggressive diuresis and his presenting symptoms improved. A biopsy of the mass was initially planned. However, paraganglioma was considered as a unifying diagnosis which could explain both his heart failure and abdominal mass. Plasma and urine metanephrines were ordered, and a biopsy was postponed until these tests resulted. Ultimately, his metanephrine levels returned markedly elevated from both the urine and plasma thereby confirming the diagnosis of a paraganglioma. Presently, the patient has unfortunately refused treatment for both his heart failure and his tumor, declining alpha-blocking medication, diuretics, and surgical management.
Discussion: Pheochromocytomas and paragangliomas are rare malignancies occurring in roughly 0.8 per 100,000 person years. They have variable presentations depending on location and character, however, the classical presentation is of hypertension, tachycardia, diaphoresis and headaches. Acute systolic heart failure secondary to catecholamine cardiomyopathy is a rare presentation of these tumors, seen in about 10% of these patients.
Conclusions: This case teaches us that pheochromocytoma/paraganglioma must be considered in the absence of classic symptoms in a patient presenting with unexplained heart failure and a retroperitoneal mass