
Background:
The Pneumonia Severity Index (PSI) is a validated risk assessment tool that estimates inpatient mortality in patients with community‐acquired pneumonia (CAP). Various clinical predictors of risk are converted to a weighted point score, which stratifies patients into 5 risk classes. Mortality increases significantly in classes IV‐V.
Some use the PSI as a tool to define which patients require inpatient care. Experience shows that patients with low risk CAP (PSI classes I‐III) are frequently hospitalized, suggesting that clinical judgment supersedes the PSI as a triage tool.
A limitation of the PSI is that hypoxia is not weighted heavily enough to consistently move patients into a high risk class. Hypoxia may impact the decision to admit patients with a low PSI score.
Method:
Retrospective study of all patients with CAP admitted to an academic medical center via the emergency department over a 6 month period (N = 93). PSI scores were calculated by chart review. Data on length of stay (LOS), intensive care (ICU) or step‐down unit (IMU) days, inpatient mortality, and nontraditional discharges (defined as discharge to acute, subacute or residential care facility or with home health services) were collected. Patients with PSI score I‐III were classified as low‐risk (LR) and IV‐V as high‐risk (HR).
Groups were then reassigned based on need for supplemental oxygen on admission and outcomes were reassessed. All patients with PSI scores of IV‐V, and scores of I‐III with an oxygen requirement were assigned to the modified high‐risk group (MHR). The rest were assigned to the modified low‐risk group (MLR).
Summary of Results:
Table 1 illustrates hospital outcomes by PSI category. As expected, the PSI score accurately predicted inpatient mortality (p = .02), but significance was lost after adjustment for oxygen requirement (p = .12). No differences in LOS or ICU/IMU days were noted. Nontraditional discharges were higher in HR patients regardless of oxygen status (p≤.01).
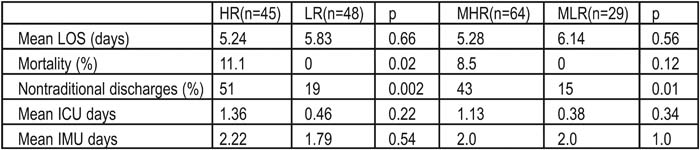
Table 1. Hospital Outcomes by Risk Class
Statement of Conclusions:
Adjustment for oxygen requirement did not overcome the limitations of the PSI as a tool to determine site of care for CAP. Outcomes other than mortality were equivalent regardless of PSI, except that nontraditional discharges were more frequent in HR patients. Clinical judgment remains superior to the PSI.
Author Disclosure Block:
G. Seymann, None; K. Barger, None; E. Fink, None; D. Davis, None; T. Dam, None; G. Maynard, None; S. Sawhney, None; S. Choo, None.