Background:
With the costs of health care rising in the US, a renewed focus on decreasing unnecessary utilization is crucial. Catheter-associated urinary tract infection (CAUTI) is a common and preventable cause of morbidity and mortality in hospitalized patients. Urinary catheter (UC) use is a risk factor for CAUTI. SHM and ABIM Choosing Wisely recommendation of “Don’t place, or leave in place, urinary catheters for incontinence or convenience or monitoring of output for non-critically ill patients” was the focus of our project to decrease CAUTI.
Purpose:
Our goal of this project was to reduce CAUTI rate by increasing awareness and identification of UC and encouraging early removal.
Description:
“Lose the Tube” quality improvement initiative was implemented at Mount Sinai Hospital on 5 medicine units. Hospitalist unit medical directors utilized the electronic medical records system to identify patients on their units with UC. During daily multidisciplinary rounds, they asked each provider with identified UC a short, simple, non-threatening question: “Does the patient need the Foley?” In addition, an educational mnemonic “NO TUBE” was developed to assist the medical directors in remembering the only acceptable indications for UC.
Neurologic (spinal/pelvic) trauma
Obstruction/Retention
Tenuous (critically ill CHF or AKI)
Urological surgery
Bed sores + incontinence
End of life
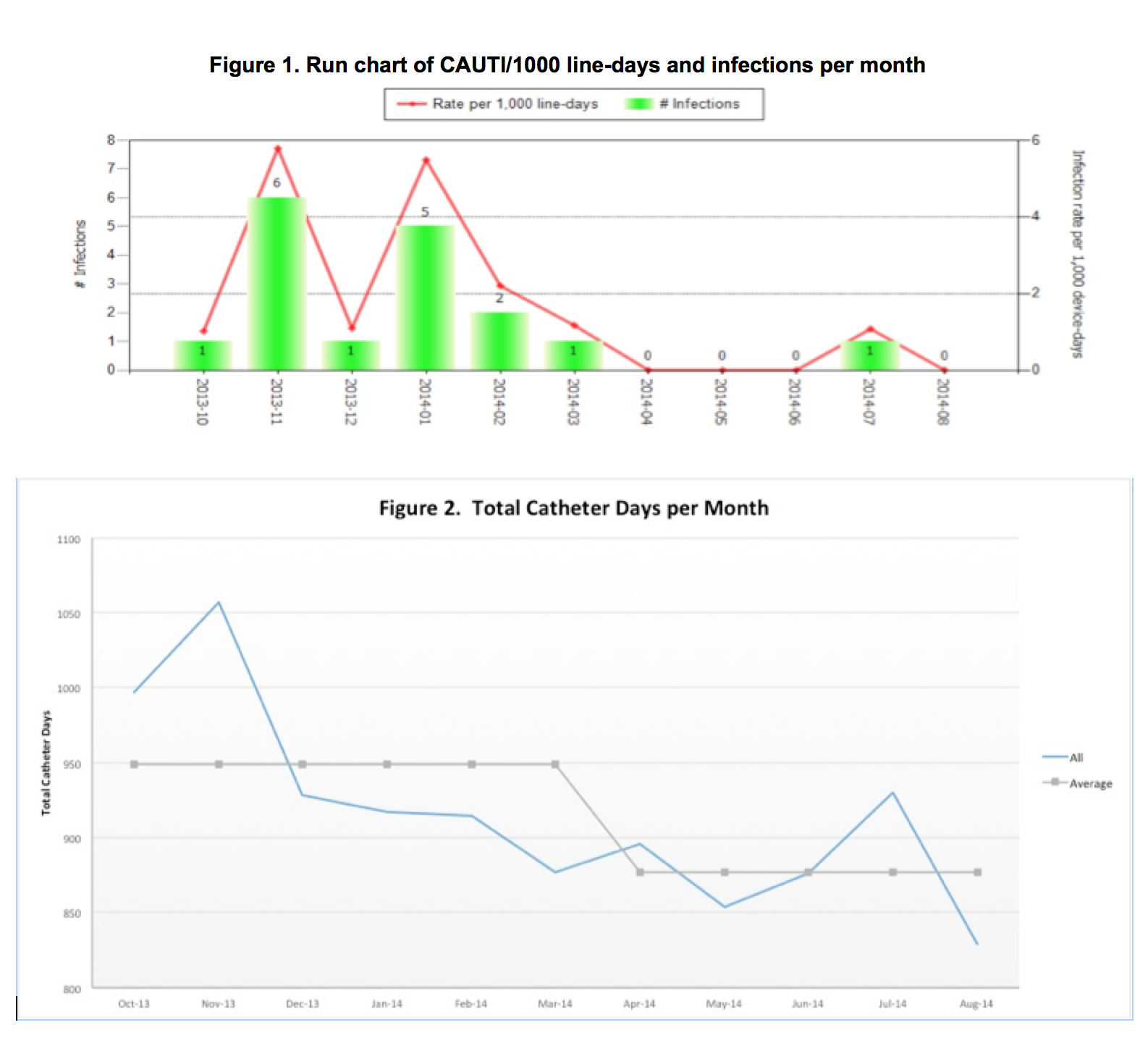
Baseline data was measured from 10/1/13 – 3/31/14 (6mos). Intervention period started from 4/1/14–8/31/14 (5mos), when the last preliminary data was collected prior to submission. Total catheter days and CAUTIs were measured, per CDC definitions.
Conclusions:
The results showed that the number of CAUTIs decreased from 16 to 1, or 2.670 CAUTI/month to 0.200 CAUTI/month (p=0.047, 95% CI 0.049, 4.884) [see Figure 1]. CAUTI rate decreased from 2.85 CAUTI/1000 catheter days to 0.23 CAUTI/1000 catheter days (p=0.001, 95% CI 1.232, 4.009). The total catheter days decreased from 5610 to 4318, from 948.50 catheter days/month to 877.00 catheter days/month (p=0.028, 95% CI 900.81, 924.69) [see Figure 2]. The estimated hospital cost savings was $2,386.82 per month for symptomatic CAUTIs alone (total $11,934.10), or $10,018.88 per month for blood stream infections alone (total $50,094.40). The projected 1 year cost savings range from $28,641.84 to $120,226.56.
The “Lose the Tube” project was effective and innovative for a few reasons. First, our intervention allows for easy identification of UC, and the interaction between the medical director and the clinician at multidisciplinary rounds is brief, effective and seamlessly integrated into existing workflow. The simple question “Does the patient need the foley?” avoids a culture of blame and instead allows ownership of the provider to make the responsible decision of removing unnecessary UC, thus avoiding a top-down approach in stewardship. It was also innovative in that it was effective without nursing engagement or emergency department engagement.