Case Presentation:
An 82-year old male presented to emergency department with complaints of severe “prostate” pain with movement, defecation, and micturition for several months, with increase in pain severity 2 weeks prior to presentation. He had received 6 days of ciprofloxacin and 7 days of trimethoprim/sulfamethoxazole for presumed prostatitis without relief. On examination, he was afebrile and hemodynamically stable with a normal leukocyte count and a prostate specific antigen (PSA) of 5.6 ng/mL. Physical exam was unremarkable except for large abnormal prostate nodules. CT scan of the abdomen showed an enlarged mass measuring 6.6 x 5.9 x 6 cm with pelvic adenopathy, and innumerable hypodense hepatic lesions concerning for metastatic disease. Patient underwent transurethral resection of prostate and rigid proctoscopy by urology service with resolution of his pain. Pathology of the prostatic biopsy showed poorly differentiated neuroendocrine carcinoma. Immunohistochemistry showed the tumor to be diffusely positive for synaptophysin; while, cytokeratin staining demonstrated dot-like perinuclear staining. CD20, CD3, and CD56 were all negative. CT guided biopsy of the liver showed metastatic, poorly differentiated small cell carcinoma with characteristics similar to the prostate biopsy. There was no evidence of primary or metastatic disease in the thorax or the brain. The patient was discharged home with oncology follow-up.
Discussion:
Small cell carcinoma of the prostate is a rare tumor that falls into the larger category of extrapulmonary small cell carcinoma (ESCC). These tumors, like small cell lung cancer, are aggressive and characterized by metastases to multiple organ systems at the time of diagnosis as well as associated with common paraneoplastic syndromes. ESCC of the prostate is more aggressive than the much more common prostate adenocarcinoma. Based on the Surveillance, Epidemiology, and End Results (SEER) database, incidence rate of this cancer is 0.28 per 1,000,000. Initial symptoms are similar to adenocarcinoma, such as urinary outflow obstruction, but may include paraneoplastic symptoms and commonly distant metastases. PSA is of limited benefit in prostate ESCC and may be elevated or low. Prior case reports suggest that prostate ESCC is commonly associated with previous adenocarcinoma treatment and a normal PSA.
Conclusions:
Small cell carcinoma of the prostate is a rare, but aggressive disease. Clinicians should consider this entity when common prostate symptoms present with unexplained paraneoplastic or metastatic symptoms. Unfortunately at time of diagnosis, prostate ESCC has commonly metastasized portending poor prognosis..
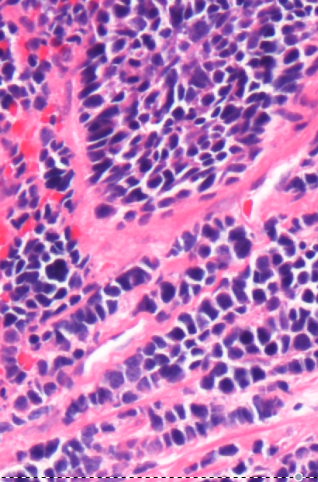
(Caption) Small Cell Carcinoma with sheets of dark blue cells with minimal cytoplasm