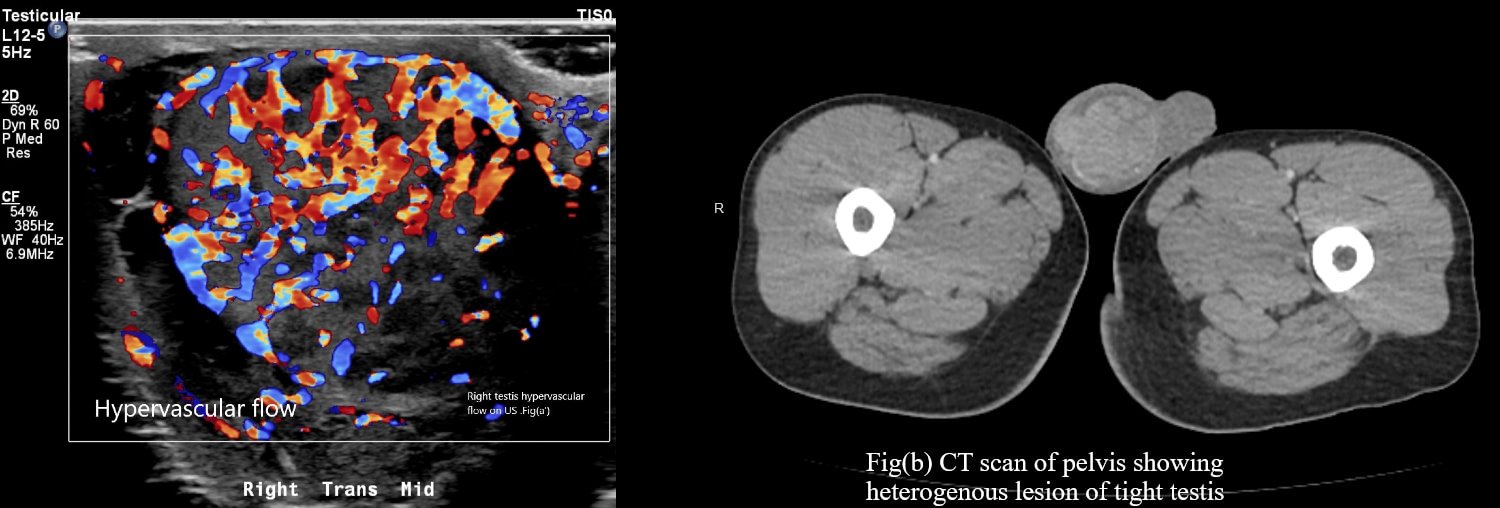
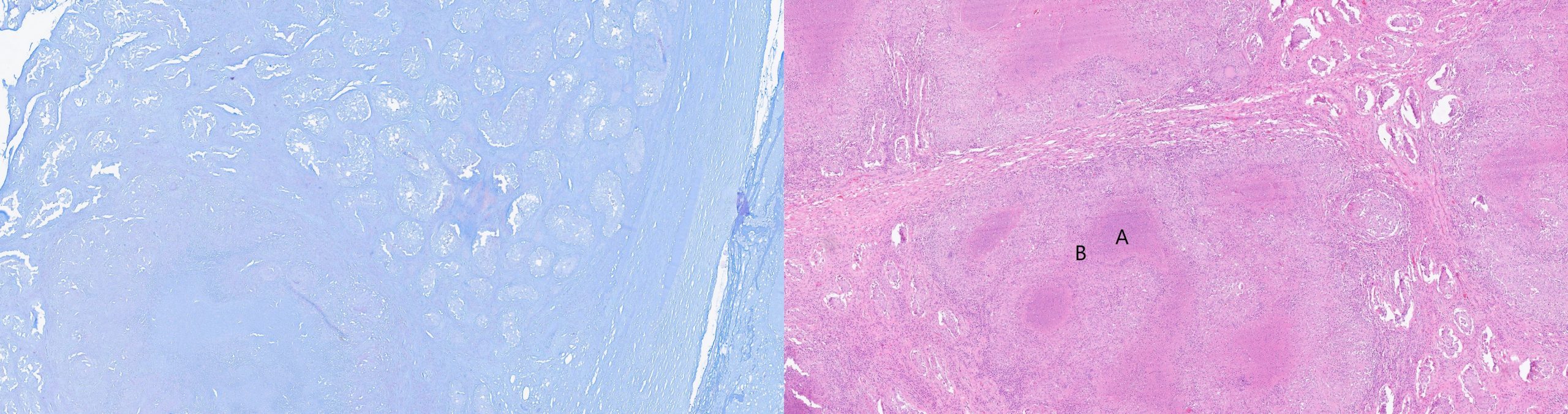
Case Presentation: A 27-year-old male immigrant male from Guatemala presented with complaint of right-sided scrotal pain, swelling, and fever of 1 month. No reports of weight loss. Physical exam revealed right scrotal swelling, induration with the tenderness of the right testis and epididymis. Lab workup showed normal CBC, CMP. Urine culture, blood culture, chlamydia, and gonorrhea urine PCR were negative. Empirical intravenous antibiotics were started for suspected bacterial epididymo-orchitis but the patient continued to have fevers. HIV serology was non-reactive. AFP, beta-Hcg, and LDH were normal. A chest X-ray did not show any abnormal findings. AFB stain from sputum was negative. CT chest abdomen pelvis showed extensive lymphadenopathy and heterogenous right testes. A right radical orchiectomy was done for suspected right testicular malignancy. Histopathology exam and AFB stains revealed Mycobacterium tuberculosis orchitis. The patient’s fever resolved after initiation of anti-tuberculous therapy.
Discussion: Isolated tuberculous epididymo-orchitis is a rare manifestation of vast extrapulmonary tuberculosis (EPTB) disease spectrum [1], especially in the developed nations, making it prone to delayed or misdiagnosis and inadvertent orchiectomy [2][3][4]. Several observational studies and case reports have been reported with the successful use of FNAC in diagnosing tuberculosis orchitis and thus avoiding inadvertent orchiectomy [5-10]. However, there is a lack of consensus for the use of FNAC for diagnostic purposes in such patients, and because tuberculous orchitis can mimic testicular neoplasm [11-15], the use of FNAC is not prevalent in developed countries with fear of seeding of tumor cells. Handa et al. and Gupta et al., in their retrospective analysis of combined more than 250 patients, found FNAC useful in 90 percent cases for diagnosis of tuberculous orchitis [5,7]. Viswaroop et al. reported a case series of 40 patients with epididymal tuberculosis in which 26 patients diagnosed with FNAC, nine patients required tissue biopsy, and five patients underwent orchiectomy for suspicion of the testicular tumor and diagnosed with histopathology specimen [10]. It has been observed that the theoretical risk of seeding of cancer to skin and lymph nodes with FNAC usually precludes its use; however, the seeding of tumor cells with FNAC remains unproven. Shah et al., in his research, reported a 95% non-neoplastic lesion in their study of epididymis nodule with FNAC [9].
Conclusions: Our case report illustrates the diagnostic challenges associated with an atypical and rare presentation of the EPTB. The condition has been long recognized and well-illustrated in the medical literature. However, it remains mostly unknown, especially to physicians trained in the developed nations due to its relatively low prevalence. Currently, available literature has demonstrated the safety and efficacy of FNAC in diagnosing TB epididymo-orchitis. We believe that the risk of the spread of tumor cells is overestimated. Hence the benefits of differentiating TB epididymo-orchitis from testicular malignancy using FNAC exceeds its minimal risk and must be considered as a diagnostic tool in evaluation.