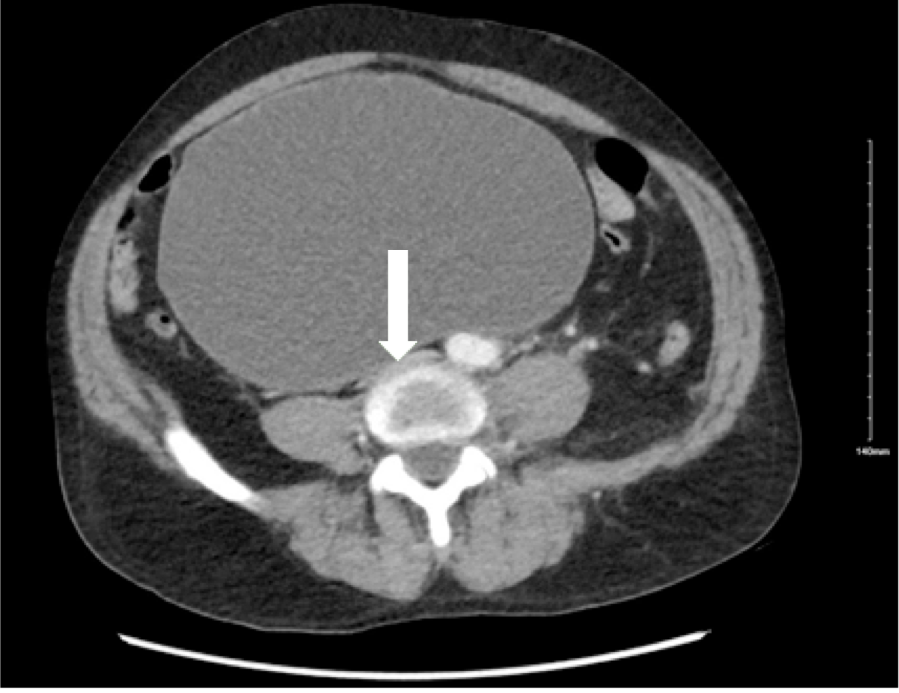
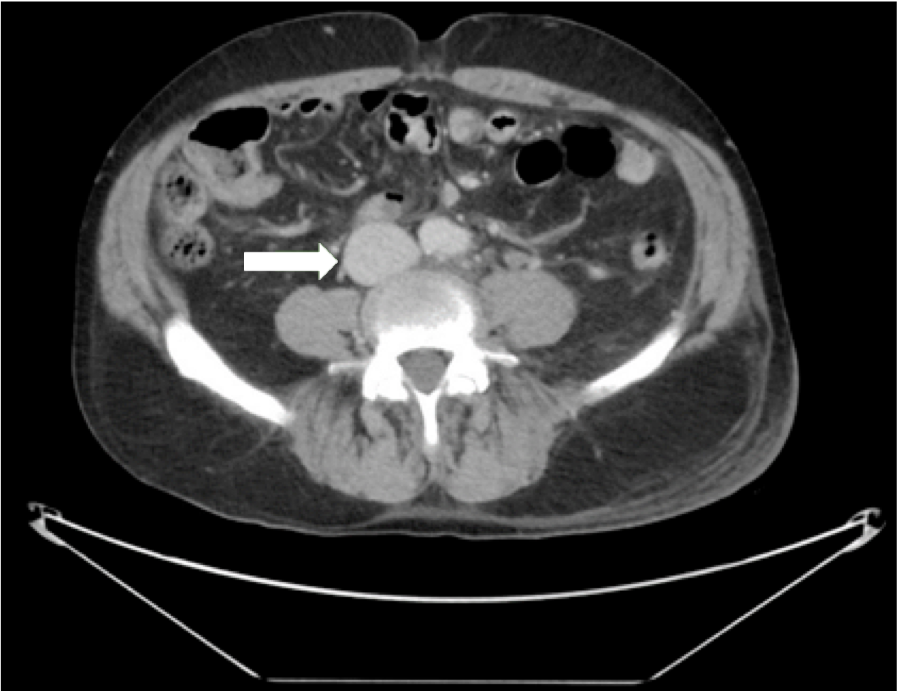
Case Presentation: A 62-year-old male with a history of Parkinson’s disease presented with worsening left leg pain and swelling for approximately one month. The patient denied any history of immobility, recent travel, malignancy, or history of blood clots or thrombophilic disorders. Physical exam was remarkable for massive abdominal distention and marked swelling of the entire left lower extremity, being more pronounced in the thigh. Labs showed leukocytosis at 19000/µL with normal hemoglobin, platelets, and coagulation panel. A duplex ultrasound revealed an extensive deep vein thrombosis (DVT) extending from the left distal femoral vein through the external iliac vein. A computed tomographic angiographic (CTA) scan of the abdomen and pelvis showed a markedly distended bladder, with the dome of the bladder 24 cm above the pubic symphysis causing significant mass effect on the distal inferior vena cava (IVC) (Figure 1) and an occluding thrombus in the left common iliac, left external iliac, left internal iliac, and visualized proximal left thigh veins. The patient endorsed having urinary hesitancy and incomplete bladder emptying for over a year and now received the diagnosis of benign prostatic hyperplasia (BPH). Treatment was initiated with placement of a urinary catheter, Tamsulosin 0.4 mg once daily, and heparin drip which was later transitioned to 10 mg Apixaban twice daily. After treatment, CT urography showed decompression of the urinary bladder with significantly reduced mass effect on the IVC (Figure 2). The patient underwent transurethral resection of the prostate (TURP) several months later.
Discussion: In this case, we describe a less common but significant cause of a DVT: urinary bladder distention secondary to BPH compressing the IVC. The first case of bladder distention causing DVT was reported in 1960 in a male pediatric patient. Thereafter, over the next 60 years, only a handful of cases of bladder distention causing DVT have been reported. The causes of bladder distention in these cases have been noted to be BPH, prostate cancer, and neurogenic bladder, with BPH being the most common cause. Elderly patients may not actively endorse urinary symptoms if their symptoms are not too debilitating, making it important for hospitalists to perform a focused history and physical exam to uncover urinary retention.
Conclusions: Urinary bladder distention from BPH can cause venous compression and stasis leading to a DVT. When investigating the underlying cause of a DVT in a patient, hospitalists should perform a focused history and physical examination assessing for urinary retention. If the suspicion is high, advanced diagnostic imaging must be done to visualize bladder distention and venous compression.