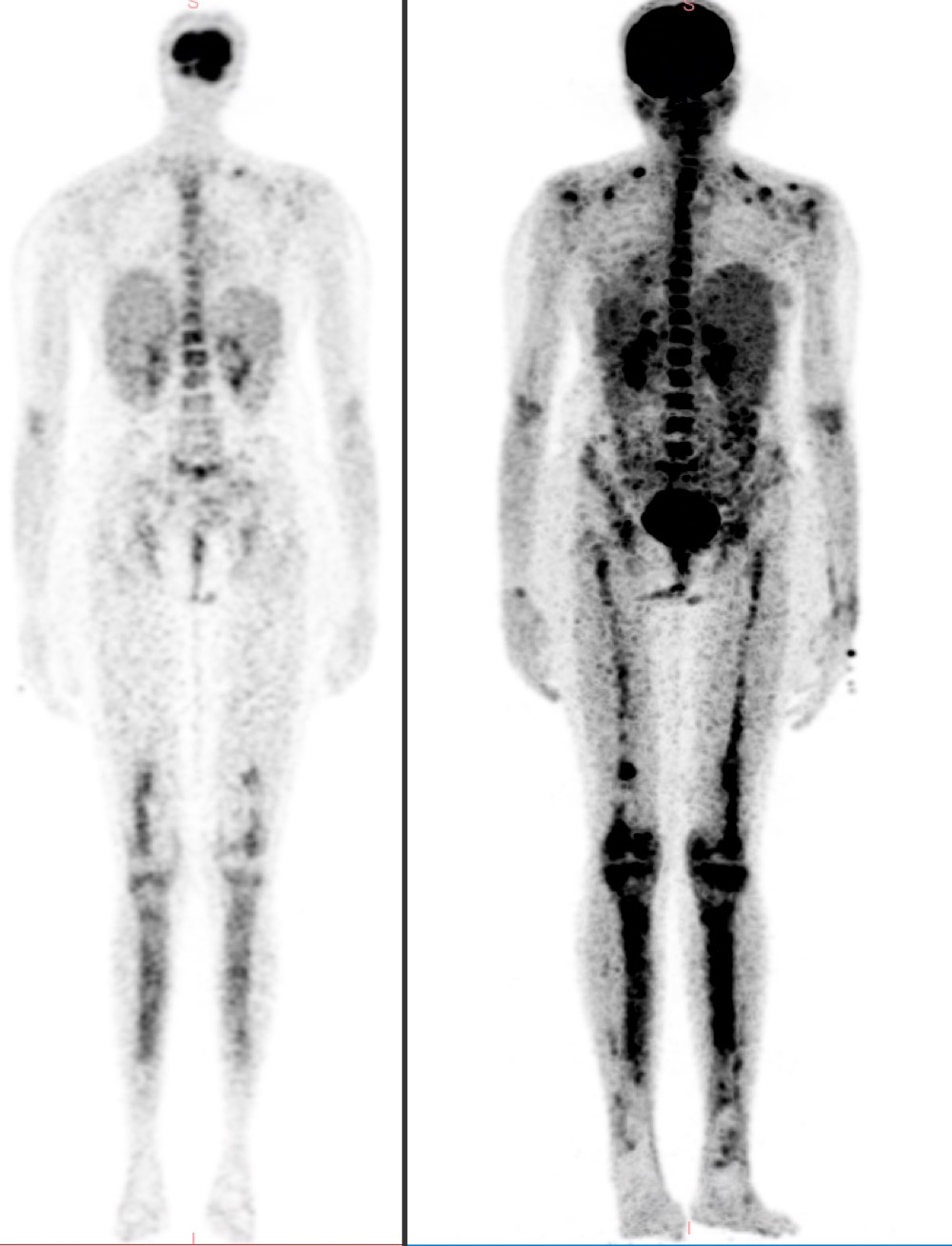
Case Presentation: Ghosal hematodiaphyseal dysplasia (GHDD) is a rare autosomal recessive disorder presenting with myelophthisic anemia and distinctive bony changes. TBXAS1 gene encodes Thromboxane A synthase. In GHDD, dysregulation of TBXAS1 occurs and this increases prostaglandin synthesis and causes direct bone marrow injury. Here we report, a 31-year-old Southeast Asian female presented with bilateral knee pain for four years. She has a history of chronic iron deficiency anemia (Hemoglobin 6.1 gm/dl). Autoimmune panel was negative. CT scan of the lower limbs (as shown in figure 1) showed multilamellated endosteal thickening involving diaphyses with severe narrowing of medullary canal. PET CT scan of lower limbs (as shown in figure 2) revealed tubular remodeling, intramedullary ground glass matrix, and mild cortical thickening. Bone marrow biopsy revealed fibrocellular marrow with dyserythropoiesis. The patient underwent a comprehensive workup for bone marrow sclerosis. Next Generation Sequencing for GHDD revealed homozygous p.Arg412Gln (exon 11) in TBXAS1. Recent evidence shows NSAIDs are effective because they inhibit COX-1 and COX-2 of the arachidonic acid pathway, prevent prostaglandin synthesis, and thus restore hematopoiesis. The patient was started on PO Aspirin 150 mg/day and at a 3-month follow-up visit, the patient reported resolution of symptoms (Hemoglobin 11 gm/dl).
Discussion: GHDD being diagnosed in adults is rare with limited genetic information available [1–3]. Our study presents a homozygous mutation in exon 11 of the TBXAS1 gene, specifically p.Arg412Gln, which has not been previously reported. Dysregulation in thromboxane synthase (TBXAS1 gene) leads to increased prostaglandin H2 production, causing the absence of osteoclastic differentiation and activation and resulting in bone marrow sclerosis. Symptoms in adults manifest as pain in weight-bearing joints or widening of the extremities. Radiological investigations show expansion and sclerosis of the diaphysis of long bones with widening of medullary cavities and cortical hyperostosis [4] and skull base involvement [5]. Hematological manifestations span from mild myelophthisic anemia and thrombocytopenia to severe pancytopenia [5,6]. The diagnosis of hemato-oncologic conditions involving the bone marrow can be identified through PET-CT scans [7]. Hypocellularity, myelofibrosis, or decreased erythroid precursors are seen in bone marrow biopsy [2,8]. Previously, GHDD was treated with prednisone of varying dosages [2,4,8] but no standard regimen has been formulated yet [7]. Brown et al postulated that NSAIDs can be used as a safer first-line therapy for GHDD. An improvement in hematological parameters and inflammatory markers was noted with the daily use of NSAIDs (Aspirin 325 mg or ibuprofen 30 mg/kg) [2,5,9,10].
Conclusions: Strong clinical intuition and complete scrutiny of radiological evidence are paramount to arriving at a diagnosis for adult onset GHDD. Despite its rare incidence, the treatment involves a simple over-the-counter NSAIDs (such as Aspirin or Ibuprofen). This is highlighted in our case report which provides a groundbreaking example of using low-dose NSAIDs as a first-line therapy for GHDD.