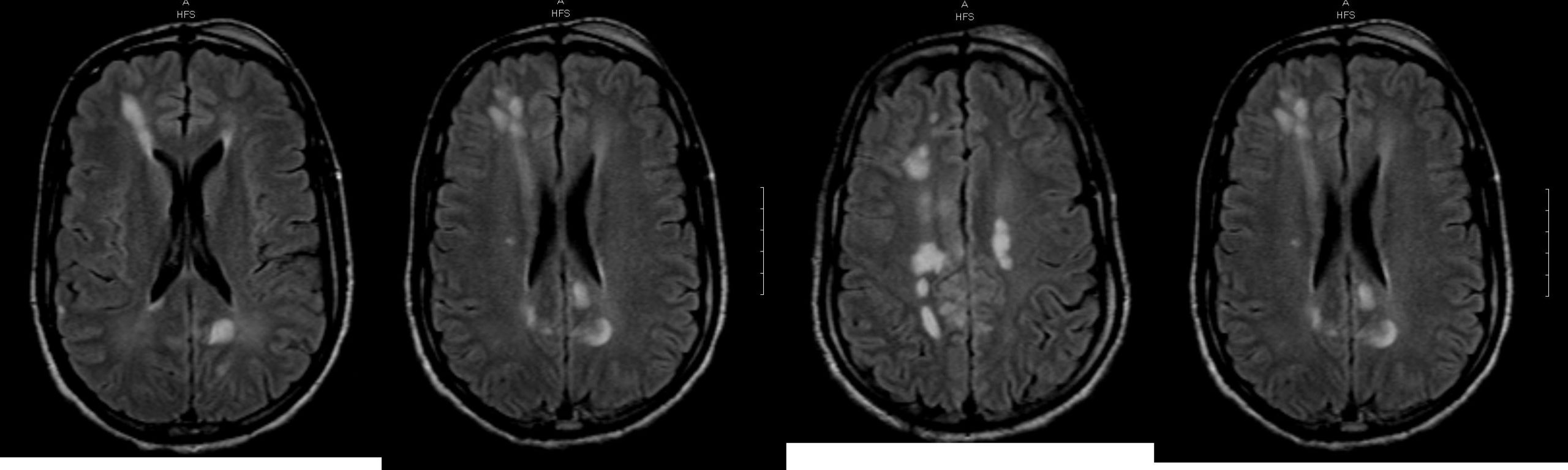
Case Presentation: A 37-year old male with PMH of HIV on HAART presented with episodes of seizure, syncope and altered mental status. Vital signs and physical examination were unremarkable. Laboratory results revealed sodium level 113, serum osmolarity 243, urine osmolarity 429 and urine sodium 113. Lab findings along with patient appearing euvolemic on exam suggested SIADH as the cause of hyponatremia. CT head showed multiple foci of abnormally decreased density within the white matter with a frontal predominance. MRI revealed multiple ovoid T1 hypointense and T2 hyperintense lesions within the supratentorial subcortical and deep white matter suggesting HIV related encephalopathy with another highly likely differential being a cryptococcal infection. Whole infectious workup including CSF analysis, cryptococcal antigen, and toxoplasma antibody was negative. Also the appearance of lesions on MRI was not typical for progressive multifocal leukoencephalopathy, tuberculosis, or lymphoma. Nephrology as well neurology input was obtained and since no other etiology for SIADH was found, this was attributed to HIV related encephalopathy changes found in his brain. Despite these changes in the brain, the patient did not have any neurocognitive impairment or dementia. With treatment of his SIADH, the patient’s mentation improved and he was ultimately discharged.
Discussion: SIADH was first described in 1957 in patients with bronchogenic carcinomas. Since then, the condition has been found to be associated with a number of disease processes including CNS disturbances, pulmonary infections, malignancies, endocrine disorders as well as certain drugs. ADH is synthesized by neuroendocrine neurons in the hypothalamus. It is transported via axons to the neurohypophysis and released into the bloodstream. In patients with HIV, cases of SIADH have been seen to be secondary to CNS infections like Mycobacterium tuberculosis, Cryptococcus neoformans, Plasmodium falciparum, or cerebral toxoplasmosis, pulmonary infections like pneumocystis carinii pneumonia or malignancy. This case illustrates the rare mechanism of SIADH caused merely by HIV related encephalopathy. It has been postulated that any central nervous system (CNS) abnormality can enhance ADH release from the pituitary gland, leading to SIADH. Similarly, the white matter abnormalities caused by HIV in our patient lead to the development of SIADH.
Conclusions: Hyponatremia in human immunodeficiency disease (HIV) and AIDS occurs in 20-80% of hospitalized patients. In a patient with HIV, hyponatremia due to SIADH is a frequent complication of opportunistic brain infections or mass lesions like lymphoma. Our case exemplifies an extremely rare and unique case of SIADH with HIV encephalopathy as the etiology. The mechanism behind this excessive ADH release is poorly understood. Further studies are needed to elaborate on the pathophysiology of SIADH in HIV encephalopathy.