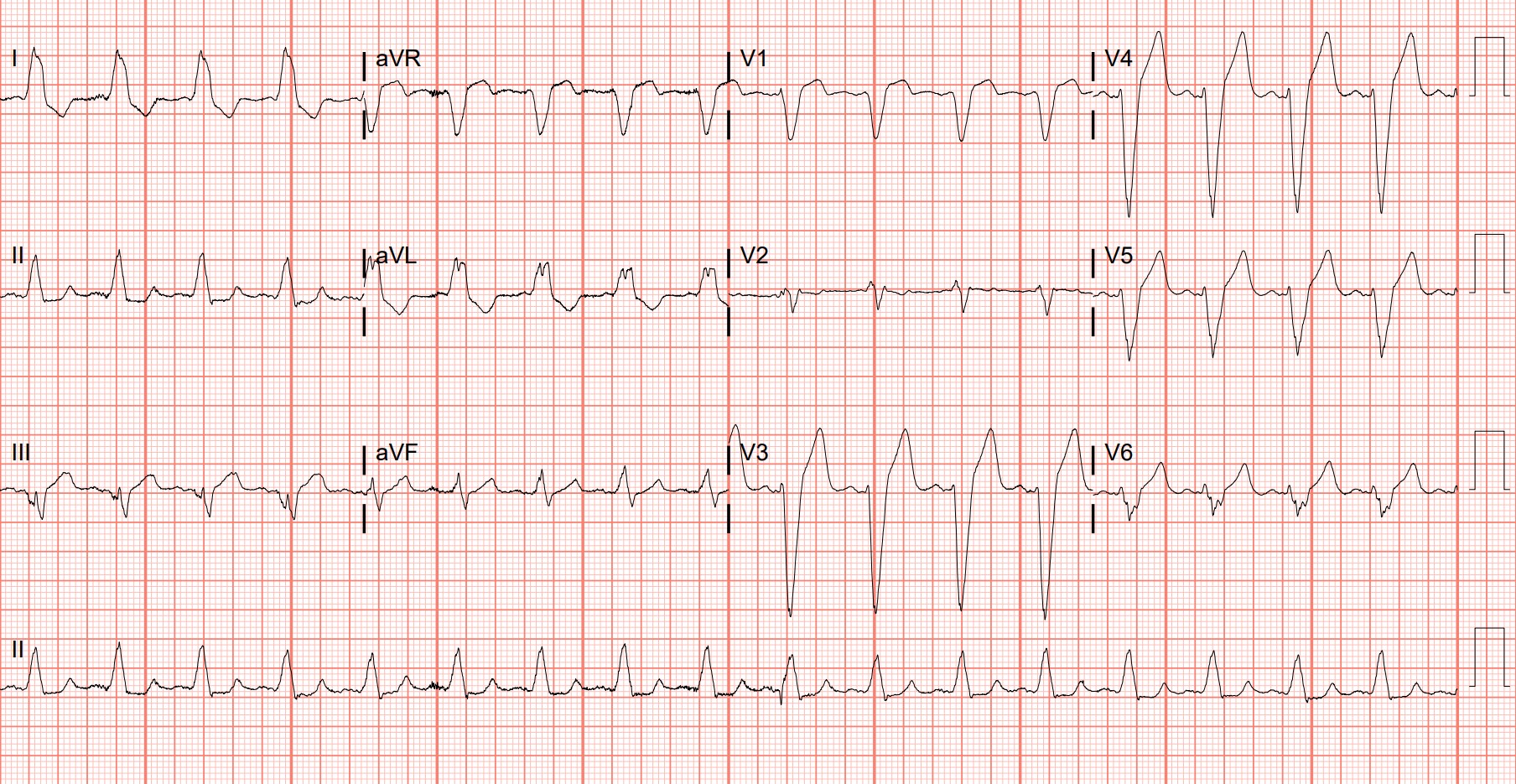
Case Presentation: A 46-year-old male with a history of HFpEF on Entresto presented for fatigue, lymphadenopathy, and severe back pain. He was diagnosed with Renal Cell Carcinoma (RCC) and was pending oncologic evaluation. On admission, his potassium and platelet levels were within normal limits. However, within the next two weeks, those levels would rise. Potassium rose from 4.7 to 6.0 g/dL in the span of days. EKG showed peaked T wave morphologies (Figure 1). He was started on Lasix and Lokelma and received many insulin shifts during this period. The patient complained of worsening flank pain during this time, and his platelets also rose to 810 x 10^3/uL. Differentials included spontaneous tumor lysis syndrome (TLS), hemolysis, and a side effect from Entresto. TLS, hemolysis, daily labs and urine studies were all normal, and Entresto was stopped. However, despite about a week’s worth of interventions, his potassium level remained elevated at 5.8 g/dL. Patient complained of feeling dehydrated due to urinating frequently, and experienced some muscle cramping. Nephrology was consulted due to concerns of needing dialysis due to persistent hyperkalemia. Nephrology noticed the thrombocytosis and requested the primary team to obtain a plasma potassium level in a heparinized test tube. The result was a potassium level close to 4 g/dL, and pseudohyperkalemia was then diagnosed. The patient’s thrombocytosis had resolved with IV fluids and optimizing his pain regimen. Within the next few days, his potassium levels had normalized. He did well afterwards and was then discharged.
Discussion: Pseudohyperkalemia was likely the result of the patient’s thrombocytosis. Platelets are considered acute phase reactants, and in a patient with RCC under significant pain and stress, his platelets were elevated. It is possible that when his blood work was drawn, due to the increased platelet numbers, clumping occurred inside the vial which lead to a leakage of K+ ions out of platelet cells which then lead to a falsely elevated K+ level. Thus, obtaining blood in a heparinized vial and preventing the clumping allowed us to correctly assess a patient’s true potassium level.It is also important to distinguish that the patient had received days of interventions, and yet the patient still had a potassium level of 4 g/dL. It cannot be excluded that this patient had true hyperkalemia in the setting of pseudohyperkalemia as depicted by the peaked T-waves on EKG. As other lab studies were normal, it is possible that Entresto caused the hyperkalemia. Once the hyperkalemia resolved, only the thrombocytosis and pseudohyperkalemia remained which was resolved soon after.
Conclusions: This vignette is important to illustrate a few points: the necessity of evaluating all causes of abnormal lab work, the relationships between blood work, and to discuss the safety of prolonged interventions regarding electrolytes. Usually, we do not place much emphasis on platelets unless they are extremely low or elevated. And when elevated, we usually do not consider its effects on other lab works. In addition after about a week’s worth of interventions, the patient had a safe level of potassium. Should the patient have had severe hypokalemia, the patient could have experienced nausea, vomiting, and in severe cases, respiratory failure due to the treatments above. Physicians always need to be cognizant and to critically think of all possible etiologies and the risks of extended interventions especially in cases of electrolyte imbalances.