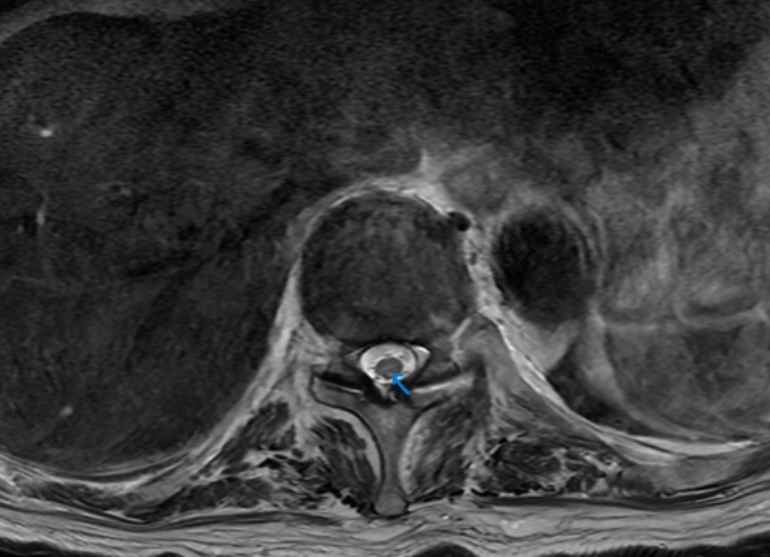
Case Presentation: A 96-year-old previously healthy Japanese man with a history of pancytopenia presented to our ED in May 2023 with ascending numbness and paresthesia. Over 1.5 months, he steadily developed numbness and tingling that ascended to his chest level (T4). He initially presented to an outside ED and received a CT T-spine that showed multilevel spinal canal stenosis. He was deemed a poor surgical candidate for spine decompression due to his age and was discharged home.He presented to our ED 1 week later with worsening proprioception and ataxia associated with appetite loss, fatigue, and weight loss. MRI C/T/L spine showed high T2 signal abnormality in the cervical and thoracic dorsal columns concerning for subacute combined degeneration (SCD) vs copper/vitamin E deficiency. Metabolic workup showed normal TSH, HgA1c, thiamine, folic acid, and vitamins B6, B12, and E. ANA and metal screen (mercury and arsenic). His CNS demyelinating panel and MAYO encephalopathy panel were normal. His copper level was undetectable. He was diagnosed with copper deficiency myelopathy. Zinc level was mildly elevated at 129 (ULN 120) and ceruloplasmin was low. He underwent urgent infusion of copper 4 mg IV x 7 days and was transitioned to 8 mg PO daily afterwards. Two weeks later, his Cu level improved to 76 ug/dL. His sensory level improved from T4 to T10 and his proprioception improved, but he continued to have paresthesias.
Discussion: Lower extremity numbness and tingling is a common complaint for hospitalists. Vitamin deficiency and diabetic neuropathy are common causes, but copper deficiency can be an unusual etiology. This case emphasizes that delayed diagnosis can result in a severe and consequential myelopathy. Copper is an essential trace element and critical cofactor for many enzymes involved in energy production, hematopoiesis, iron metabolism, neurotransmission, and connective tissue maturation. Copper is prevalent in shellfish, nuts, seeds, and meat. There are several common causes of deficiency. Because copper is absorbed in the duodenum, bariatric surgery, proximal bowel resection, and Celiac disease can cause deficiency. Excessive zinc intake, either through denture adhesive use or oversupplemention, can also result in deficiency. Both copper and zinc are competitively absorbed by metallothionein in intestinal cells. Excessive zinc causes upregulation of metallothionein, which has a higher affinity of copper, trapping copper and depleting stores. Notably, this patient had never had abdominal surgery, ate healthy, and did not use adhesives or take zinc supplements.The mechanism of axonal destruction remains unclear. The T2 hyperintensity seen in dorsal columns on MRI mimics SCD. Copper deficiency is also associated with pancytopenia that mimics MDS. Bone marrow biopsy reveals decreased granulopoiesis and iron containing plasma cells. Our patient had pancytopenia but declined bone marrow biopsy for further diagnosis.Copper deficiency is an under-diagnosed syndrome with profound neurologic and hematologic consequences. Repletion can result in neurological and hematological symptom recovery, as highlighted in this patient’s course.
Conclusions: Copper deficiency is an underdiagnosed cause of lower extremity numbness. When left untreated, it can progress to profound ascending myelopathy with associated pancytopenia. SCD is the main differential. Pancytopenia caused by copper deficiency often mimics MDS. Treatment can lead to symptom reversal.