Background: Increasingly, hospitalizations are becoming more complex and patients are frequently discharged from the hospital with new medical diagnoses, medications, and need for close follow up care (1,2). In 2009, the Health Information Technology for Economic and Clinical Health Act published meaningful use rules for using the Electronic Health Record (EHR), which included that the EHR should be used to provide effective health information exchange to improve health care quality and patient-centered care (3). In the inpatient setting, utilizing technology and health information tools such as through the patient portal (MyChart) can be a way for hospitals to facilitate patient engagement, increase health access, and improve patient-provider communication (4).
Purpose: The purpose of this quality improvement initiative is to increase MyChart activation and utilization for hospitalized patients at the University of Chicago Medical Center (UCMC). In doing so, we hope to facilitate patient engagement, increase patient-provider communication, and improve care transitions.
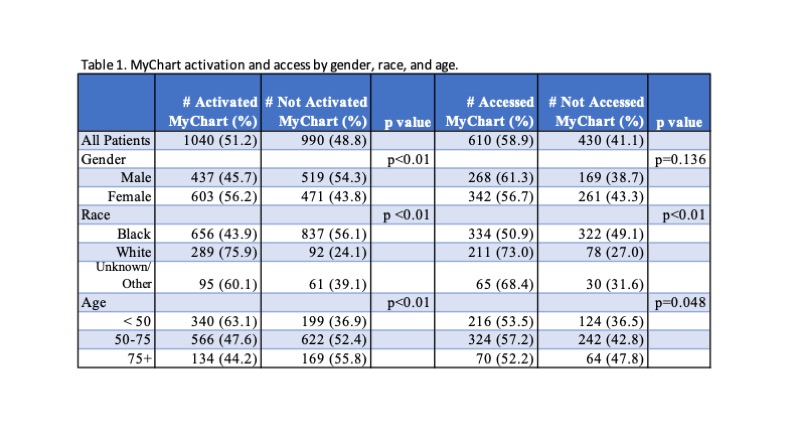
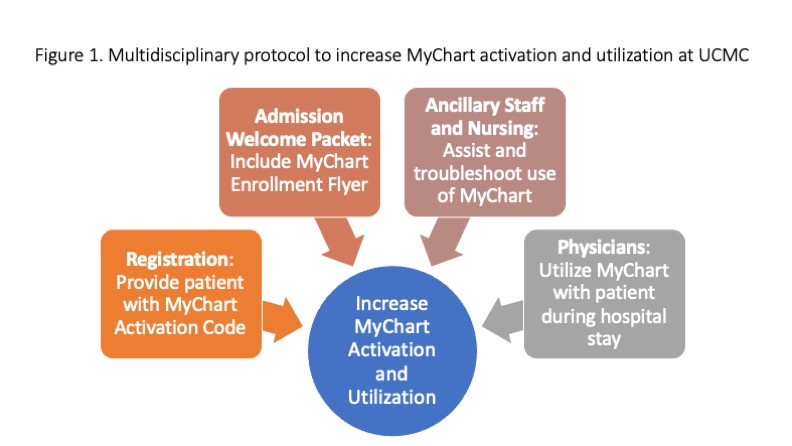
Description: We obtained baseline characteristics of activation and use of MyChart during inpatient hospitalization from the Hospitalist Project, a longitudinal research study that targets patients admitted to UCMC. Our sample covered a six-month period between 1/15/22- 7/15/22. In total, 51.2% of the enrolled patients had activated MyChart and 58.6% of those patients accessed MyChart during their hospital stay. There was a larger proportion of White patients in comparison to Black patients who activated MyChart (75.9% to 43.9%, p< 0.01). Female patients had more activations (52.9% to 47.1%, p< 0.01), and younger patients (age < 50) had more activations compared to those aged 50-75 and 75+ (63.1% to 47.6% to 44.2%, p< 0.01). These demographic trends were similar for accessing MyChart during an encounter. This shows a disparity in gender, race, and age and thus demonstrates a tremendous area to improve access for patients to their health information. Our initiative to increase MyChart activation and utilization involves a multidisciplinary approach. On admission, patients are provided with their MyChart activation code as well as information about utilizing MyChart during their stay. A hospital-wide campaign raised awareness of MyChart activation and usage for inpatients. This included education and training for ancillary staff, nursing, and physicians on activation and engaging patients and caregivers in their health with MyChart during their hospitalization. Throughout this initiative, we will be evaluating the impact of increasing MyChart portal activation on patient engagement, satisfaction, and transition of care metrics including length of stay, readmission, and attending follow up appointments.
Conclusions: Optimizing the use of technology and health information tools in the inpatient setting including the use of MyChart may help to improve patient health outcomes, healthcare equity, and digital health literacy. Pre-intervention data from our project indicates that only about half of hospitalized patients have MyChart activated and fewer have utilized MyChart during their hospitalization. Additionally, while Black patients represent the majority of patients at our urban academic center, they were found to disproportionately activate MyChart less compared to their White counterparts. These findings indicate that further emphasis on interventions that focus on health equity are needed in our urban population.