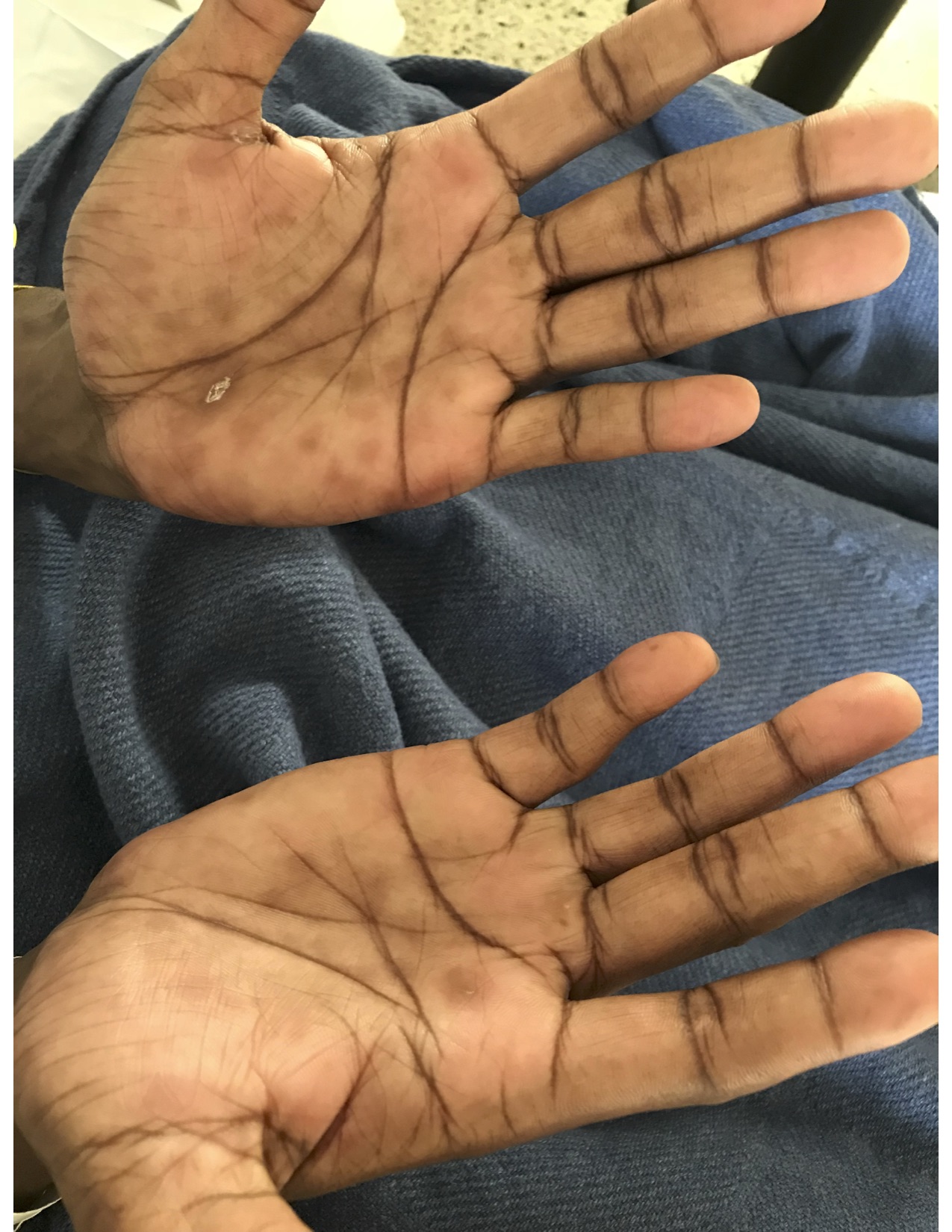
Case Presentation: A 34-year old male with a history of acquired immunodeficiency syndrome (CD4 count 268 cells/µL, viral load 31 copies/mL) and Kaposi’s sarcoma presented with two days of diarrhea, abdominal pain, and a new rash on his hands. He had unprotected sexual intercourse with a new partner a few days prior to admission. On presentation, he was febrile and tachycardic. Physical exam revealed a hyperpigmented rash on his palms and soles bilaterally and condyloma lata on rectal exam. Initial laboratory workup revealed an alanine aminotransferase of 467 unit/L, aspartate aminotransferase of 259 unit/L, alkaline phosphatase of 1255 unit/L, and a total bilirubin of 0.3 mg/dL. A rapid plasma reagin was non-reactive. Gonorrhea and chlamydia screening from the rectum was positive. Secondary syphilis was suspected due to his pathognomonic presentation despite the unreactive rapid plasma reagin. The patient’s rapid plasma reagin sample was re-run after dilution which was reactive with a titer of 1:32. The patient was treated for secondary syphilis with one dose of 2.4 million units of benzathine penicillin intramuscularly. His diarrhea was thought to be secondary to proctitis from Gonorrhea/Chlamydia, however, due to the severity of symptoms, he was treated empirically with a course of doxycycline for lymphogranuloma venereum. His symptoms improved, and liver enzymes began to downtrend. Outpatient follow up showed near normalization of liver enzymes.
Discussion: Secondary syphilis occurs in approximately twenty-five percent of individuals with untreated primary syphilis. Manifestations of secondary syphilis are varied, and can include the classic palmar and solar rash, a diffuse body rash, condyloma lata, glomerulonephritis, hepatitis, central nervous system involvement in addition to constitutional symptoms such as fever, malaise, lymphadenopathy, arthralgias, and weight loss. Syphilitic hepatitis, as seen in this case, typically presents with a disproportionally elevated alkaline phosphatase level, with normal to mildly elevated transaminase and bilirubin levels. Liver enzymes normalize after treatment for syphilis. False negative results can occur due to an antibody-antigen mismatch called the prozone phenomenon. Agglutination reactions rely on an antibody to antigen ratio within the zone of equivalence, or optimal ratio. The prozone refers to an excessively high antibody to antigen ratio, while the post zone refers to a low antibody to antigen ratio. Both can lead to false negative results, as a visible precipitant will not form properly.
Conclusions: This case demonstrates that when the clinical suspicion for syphilis is high, it is prudent to have the laboratory dilute the sample in an attempt to bring the antibody to antigen ratio into the zone of equivalence if the initial rapid plasma reagin is non-reactive.