Background: Sodium-glucose cotransporter-2 inhibitors (SGLT2i) reduce the risk of heart failure (HF) hospitalizations and cardiovascular mortality among patients with HF and left ventricular ejection fraction (LVEF) ≤40%. There is emerging evidence of the benefits of SGLT2i in HF patients with a higher LVEF (>40%). We aimed to evaluate the benefits of SGLT2i in different subgroups of patients with HF and LVEF >40%.
Methods: We searched PubMed, EMBASE, clinicaltrials.gov, Cochrane, and Google Scholar for randomized controlled trials (RCTs) comparing outcomes of SGLT2i vs. placebo in patients with HF and LVEF >40%. The hazard ratios (HRs) and 95% confidence intervals (CIs) in each study were used for the meta-analysis. The primary composite outcome (PCO) was HF hospitalization or cardiovascular mortality. Secondary outcomes included HF hospitalization, cardiovascular mortality, and all-cause mortality.
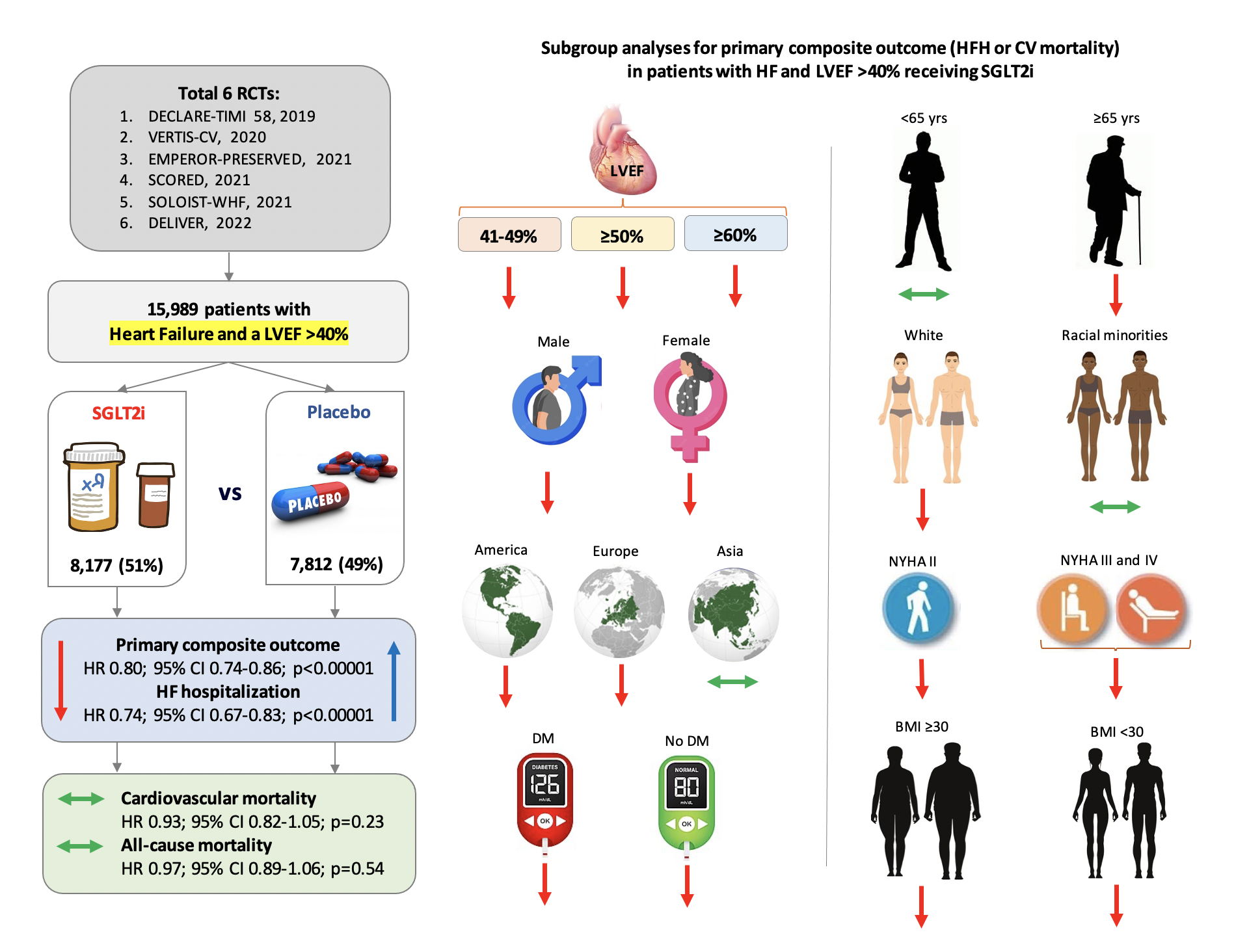
Results: Six RCTs with 15,989 patients were included (median follow-up=27.3 months, 40.8% females). In patients with HF and LVEF >40%, SGLT2i were associated with significantly lower PCO compared to placebo (HR 0.80; 95% CI 0.74-0.86; p< 0.001). This was consistent across 10/13 subgroups examined, including LVEF. SGLT2i also reduced HF hospitalization but not cardiovascular or all-cause mortality. Patients < 65 years old, from racial minorities, or from Asia receiving SGLT2i did not demonstrate a significant reduction in PCO.
Conclusions: SGLT2i significantly reduce the combined risk of HF hospitalization or cardiovascular mortality among patients with HF and LVEF >40%. However, younger patients, racial minorities, and patients from Asia did not demonstrate such a reduction. Further research is necessary to identify the reasons for such disparities.