Background: Acute Decompensated Heart Failure (ADHF) is responsible for over a million hospitalizations per year in the US and Europe. The American Heart Association Guidelines for treatment of patients hospitalized with ADHF recommend intravenous (IV) diuresis with loop diuretics to reduce fluid overload until vascular congestion is relieved. However, the optimal dosing strategy for IV diuretics remains non-standardized and the inability to predict a patient’s response to diuresis due to factors such as diuretic resistance can lead to prolonged hospital stays and poorer outcomes. Previous studies such as the Yale Diuretic Pathway (YDP) trial and the ENACT-HF trial have shown that structured, nurse-driven, titratable diuretic protocols can improve clinical outcomes in patients hospitalized for ADHF. This study aims to evaluate the impact of a nurse driven, titratable IV Furosemide protocol on hospital length of stay (LOS) for patients hospitalized with ADHF at our institution. We will also evaluate the impact of this protocol on secondary outcomes including 30-day readmission rate, relative frequency of acute kidney injury and initiation of dialysis, hypotension (< 90 mmHg), electrolyte disturbances (hypokalemia < 3 mmol/L), and time to decongestion (defined as transition to oral maintenance diuretic therapy).
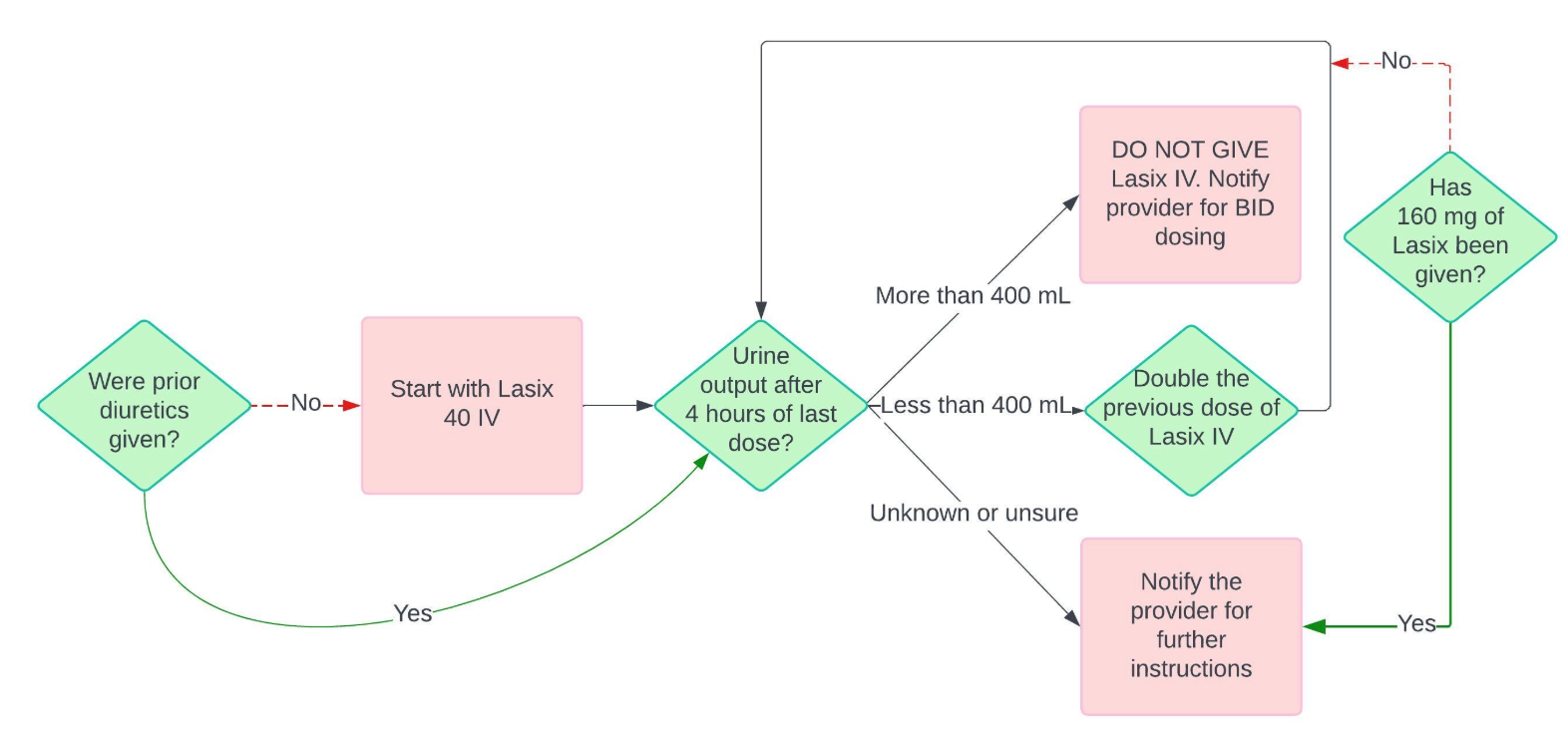
Methods: This retrospective study included 1254 patients hospitalized for ADHF at Corewell Health West – Butterworth Hospital in Grand Rapids, MI. The 1254 patients were subdivided into two groups with 880 patients in the titratable IV furosemide protocol (TIFP) group and 374 patients in the standard care group. The TIFP protocol allows for incremental titration of IV furosemide dosage by nursing staff based on the patient’s urine output over the last four hours in order to achieve optimal diuresis. Data from electronic health records was collected including demographics, diuretic dosing, urine output, fluid balance, laboratory data, treatment data, length of hospital stay, and 30-day readmission rates. A stratified, propensity-score-matched analysis comparing patients treated with the titratable IV furosemide protocol vs standard of care at our institution remains in process. Stratification will occur by heart failure type and propensity score matching will include age, race, sex, weighted DRG, relevant co-morbid conditions and relevant medications.
Results: The goal length of stay for this study was defined as 6.64 days, based on the prior average length-of-stay for patients with decompensated heart failure at our institution. Preliminary analysis of the data collected for this study revealed that the average LOS for patients receiving treatment with the titratable IV furosemide protocol was 5.73 days, which is a nearly one day reduction in length of stay. Protocol adherence by the general hospitalist team was 71.6% with a goal usage of 70%. The data for secondary outcomes is not yet available.
Conclusions: The use of our nurse-driven, titratable IV furosemide protocol for treatment of patients hospitalized with ADHF lead to a reduction in hospital LOS by about one day from the prior average LOS for hospitalized ADHF patients at our institution. This finding supports the feasibility and efficacy of structured, nurse-driven diuretic protocols in management of ADHF. A more robust statistical analysis including a stratified, propensity-score-matched analysis will be conducted to further investigate the impact of this protocol on the primary and secondary outcomes.