Case Presentation:
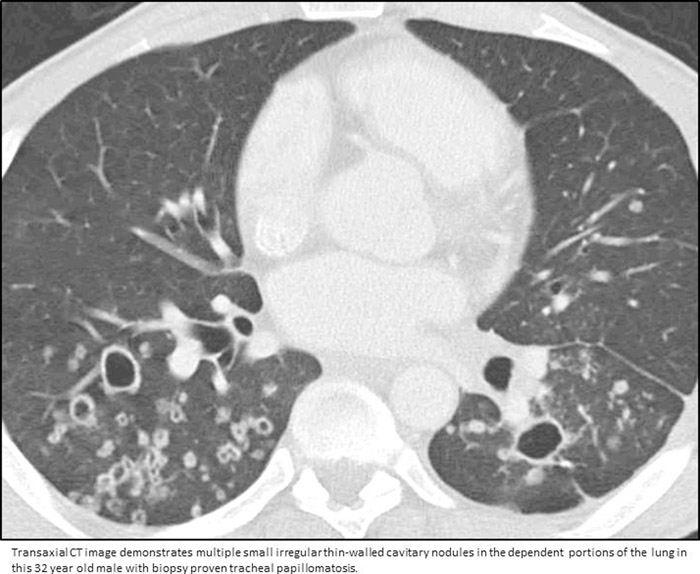
A 29‐year‐old African American hypertensive male smoker presented with hoarseness and dyspnea. He was noted to be hypoxic and was intubated. Bronchoscopy and laryngoscopy were performed with excision of extensive tracheal papillomas. Pathology testing was sent and demonstrated recurrent respiratory papillomatosis (RRP). Tissue was sent for epidermal growth factor receptor (EGFR) mutational analysis and staining. Mutational analysis was negative but EGFR immunohistochemistry was strongly positive in 80% of the cells. He was extubated two days later. Once able to be obtained, previous history revealed an episode of respiratory failure requiring intubation and tracheostomy at age 27 followed by laser debridement of respiratory papillomas with later decannulation. He had required repeat papilloma excision at age 28 and reported previous abnormal pulmonary function testing, but details were unknown. He went on to require microdebridements every two to three months, and underwent an emergent cricothyrotomy after one of the debridements because of an inability to ventilate and oxygenate. He was started on erlotinib, an EGFR inhibitor which temporarily stabilized his disease. However, follow‐up CT scans revealed growing, progressive, bilateral cavity lung lesions. At age 31, he underwent wedge resection of the left lung and bronchoscopy with transbronchial needle aspiration and biopsy. Surgical pathology showed squamous papilloma. Currently, he is still on erlotinib and continues to receive debridements. He is also suffering from intermittent hemoptysis. His multiple consultants are working on a plan to treat this difficult and rare disease.
Discussion:
RRP is caused by human papillomavirus (HPV) strains 6 and 11. Transmission is thought to be peripartum in children and sexually in adults. It has a bimodal age distribution; the juvenile form occurs mostly in ages <5 and in 4.3 per 100,000 persons, and the adult form occurs mostly in the fourth generation and in 1.8 per 100,000 persons. Most common presenting symptoms are hoarseness and dyspnea. RRP is commonly misdiagnosed as asthma, COPD, or bronchitis. These tumors involve the nose, mouth, larynx, and lungs. Remission is rare and tumors can recur even with remission. Current treatment options include serial debulking, microdebridement, intralesional cidofovir, and interferon. Use of EGFR inhibitors is being explored. At this time there is no cure. Malignant degeneration to squamous cell carcinoma is very common, almost inevitable, and carries a very poor prognosis.
Conclusions:
The purpose of this case presentation is to report a rare disease process and an up‐to‐date literature review. These patients utilize an array of medical specialists, with a hospitalist often guiding their inpatient care.