Background: Preventive care is a crucial but underutilized component of optimal population health management. Of eligible patients, 69.0% have received pneumococcal vaccine, 24.1% zoster vaccine, and 30.0% hepatitis B vaccine. Cancer screening rates are similarly low, with 12.5% screened for lung cancer and 71.6% for colorectal cancer. Gaps in preventive care are even larger in racially minoritized subgroups and those experiencing housing instability, substance use, or severe mental illness. The need overwhelms primary care to address alone. Hospital admission offers an opportunity for patients to obtain overdue preventive care.
Purpose: To increase preventive care during hospital admission in three domains: vaccinations, cancer screening, and laboratory tests.
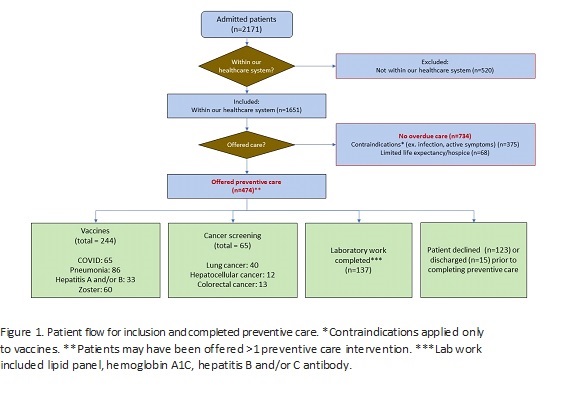
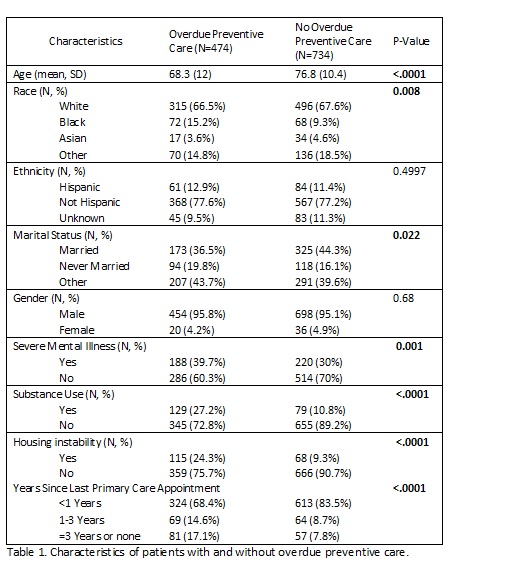
Description: We developed a protocol to evaluate inpatients for overdue preventive care and leverage the admission to complete any appropriate items. A physician lead screened inpatients on medicine, orthopedic, neurosurgery, and podiatry services for clinical reminders in three domains: vaccines, cancer screening, and laboratory tests. Vaccines included COVID, zoster, pneumonia, hepatitis A, and hepatitis B. Cancer screening included low dose computed tomography (LDCT) for lung cancer, ultrasound for hepatocellular cancer, and fecal immunochemical test (FIT) for colorectal cancer. Laboratory tests included lipid panel, hemoglobin A1C, and hepatitis B and C screening. For patients with any overdue care in these three domains, the chart was reviewed. Patients with limited life expectancy, either enrolled in hospice or undergoing discussions about hospice, were excluded. For vaccinations, the EHR was reviewed for contraindications such as infection, fever, or active symptoms. Any remaining patients were deemed appropriate to offer preventive care. The physician 1) entered orders for the inpatient care (vaccines, radiologic tests, and/or laboratory tests) 2) informed the inpatient team through secure messaging 3) followed up on the laboratory and radiographic results and 4) ordered remaining care for outpatient when applicable (ex. to complete remaining doses of a vaccination series). Over the one-year intervention period, 2171 patients were screened. The 520 patients who were not in our healthcare system were excluded. Of the remaining 1651 patients, 474 (28.7%) patients were offered at least one preventive care intervention (Figure 1). Of these patients, 321 patients received at least one preventive care intervention during their admission. Compared to the baseline period, the number of inpatient vaccinations increased by 217.9% (112 versus 244 vaccines) and lung cancer screening increased by 333.3% (12 versus 40 LDCTs).Characteristics of patients with and without overdue preventive care are shown in Table 1. Patients with overdue preventive care were more likely to be Black (15.2% versus 9.3%, p 0.008), have a diagnosis of severe mental illness (39.7% versus 30.0%, p 0.001) or substance use (27.2% versus 10.8%, p<.0001), or experience housing instability (24.3% versus 9.3%, p<.0001). Patients with overdue care were more likely to have over three years since their last primary care visit (17.1% versus 7.8%, p<.0001).
Conclusions: Preventive care can be successfully delivered to inpatients to meet the needs of underserved patients. Supplementing traditional models by offering preventive care during admission can reduce health inequities and meet the needs of a diverse population.