Background: Cross-cover, or care for hospitalized patients when the primary team is absent, is a ubiquitous yet understudied aspect of inpatient care marked by cognitive complexity. Trainees confront challenges when performing cross-cover care (1) which may be viewed through the lens of Cognitive Load (CL) Theory (CLT) (2,3). CLT is an established learning theory accounting for limits of working memory: intrinsic CL (essential to the task, e.g. complex patient), extraneous CL (not essential to the task, e.g. short staffed), and germane CL (learning related, e.g. hesitancy to seek help). The impact of CL on trainee performance has been studied in handoffs (4-6). Investigating types of CL within the challenges trainees face when providing cross-cover may improve learning and patient care if educators are able to identify strategies that decrease extraneous load and optimize germane load.Purpose: To characterize cross-cover challenges and their contributions to the CL of cross-cover.
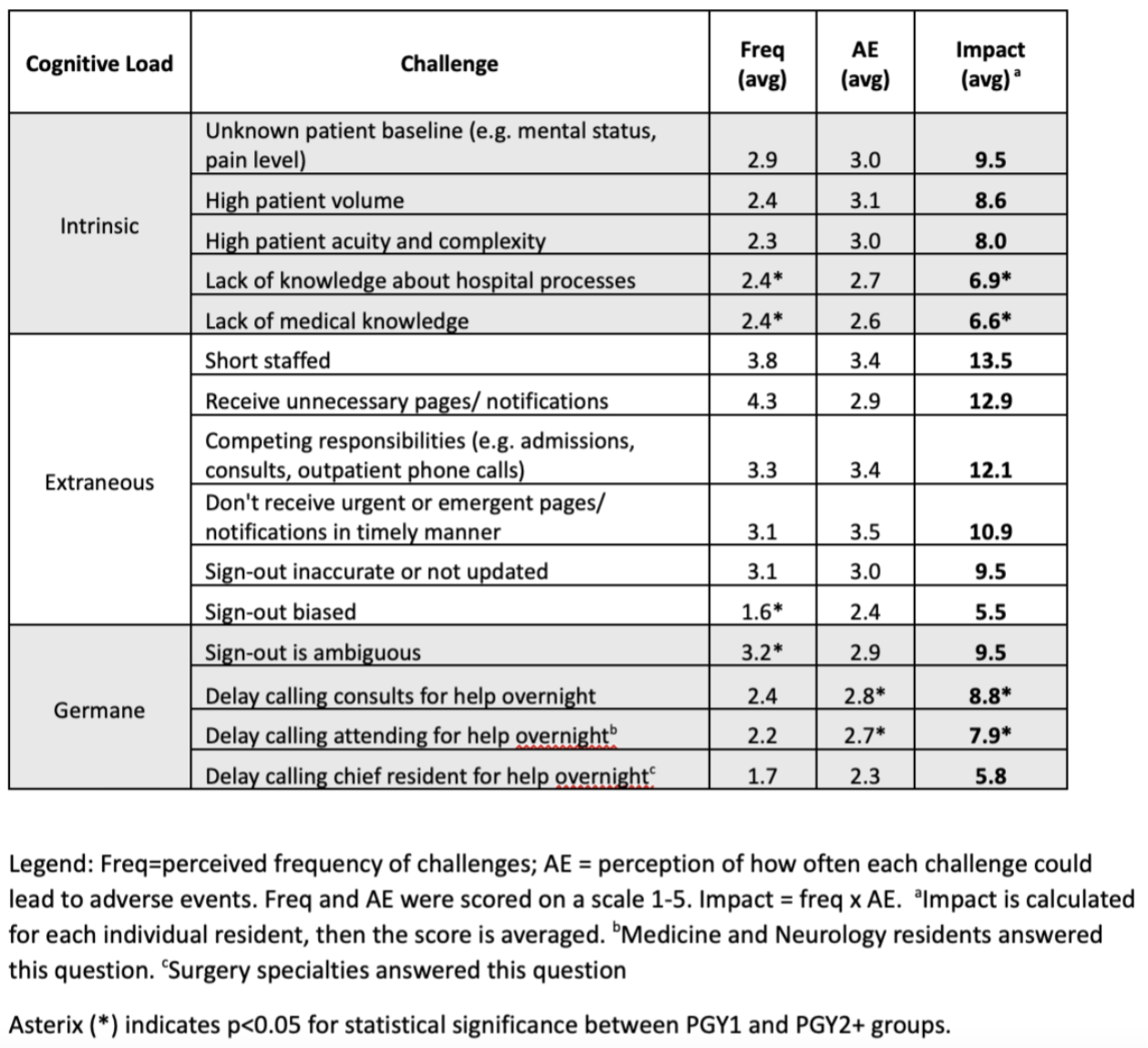
Methods: Participants included 329 trainees at a single institution in February 2023. Specialties included Internal Medicine, Medicine-Pediatrics, Pediatrics, Neurology, Surgery.Anonymous, electronic survey via Qualtrics (Provo, UT). Items were empirically developed from previous qualitative interviews (1). Pilot testing included cognitive interviews with 7 trainees to ensure response process validity and testing the survey with 12 residents to ensure optimal item flow and timing. Participants were asked to estimate the frequency of 15 challenges faced by trainees during cross-cover (1=Never, 2=Less than once every 7 shifts, 3=Once every 2-7 shifts, 4=Once per shift, 5=Multiple times per shift) and perception of how often challenges could lead to adverse events (AE, 1=Never, 2=Seldom < 10%, 3=Sometimes 10-25%, 4=Often 26-75%, 5=Almost always >75%). The challenges were previously ascertained in qualitative interviews by members of our study team (1). Impact score was calculated for the challenge by multiplying 5-point frequency scale by 5-point AE scale. Impact ranges from 1-25, higher scores indicating higher impact of the challenge on patient care. Differences between early trainees (PGY1) and more senior trainees (PGY2+) were analyzed using T-tests with significance set as p=.05 using SPSS (Chicago, IL).
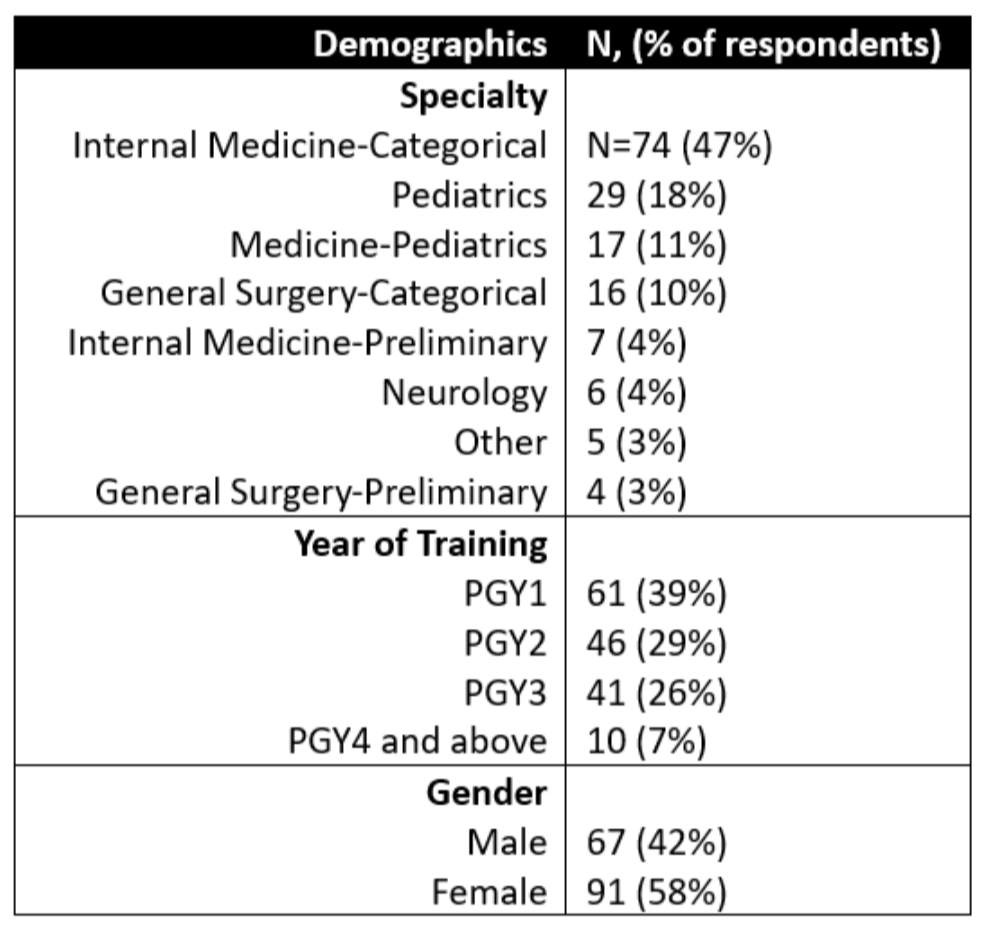
Results: Response rate was 48% (n=158). Demographics in table 1. Frequency, perception of AEs, and impact of each challenge is quantified in Table 2. Most impact is attributed to extraneous load. Differences between PGY1 vs. PGY2+ were significant for several challenges including [Average (SD)]: lack of medical knowledge [7.6 (4.2) vs. 6.0 (2.6), p=.011], lack of knowledge of hospital processes: [7.9 (3.9) vs. 6.2 (2.8), p=.006], delay calling attending overnight [9.1 (4.5) vs. 7.0 (3.1), p=.024], delay calling consultants overnight [10.8 (5.5) vs. 7.7 (3.4), p= .002].
Conclusions: Understanding CLT as it applies to cross-cover may mitigate inappropriate challenges, support learning and improve patient care. For example, reducing intrinsic load may be accomplished by titrating cross-cover responsibilities based on the experience of the learner (6). Lessons may also be applicable to improving hospitalist practice. For example, extraneous load can be reduced by improving processes, such as clearly defining the cross-cover role to decrease unnecessary notifications. Future work should focus on applying these findings to develop tailored interventions to enhance education and improve patient safety.