Background: Sepsis is a life-threatening condition involving organ dysfunction caused by a dysregulated response to infection [1]. Sepsis is the leading cause of 30-day unplanned readmissions nationwide [2]. At UF Health Shands Hospital, the 30-day readmission rate for sepsis patients is 17% compared to 13% for all adult patients. Of those readmitted for sepsis, 38% return within 7 days, underscoring the need for interventions in the first 7 days post-discharge. We developed a pilot program to evaluate the implementation of a post-discharge multicomponent program for patients admitted with sepsis, with an emphasis in telehealth. This program focuses on early detection of fluctuations in vital signs and escalation protocols to health professionals to reduce readmissions and short- term mortality.
Methods: Patients with an admission diagnosis of sepsis were recruited from the University of Florida (UF) Health Shands Hospital, a leading tertiary care center from October 2022 to August 2023. Consented individuals were then provided with a vital signs kit by a health coach along with post-discharge education, education on kit use, symptoms to monitor, red flags and follow-up for 2 telehealth visits.An age-matched control group with a diagnosis of sepsis was obtained from the Integrated Data Repository at UF. A total of 100 patients were included, maintaining a minimum 2:1 control-to-intervention ratio. The intervention group consisted of 30 patients, while the control group included 70. The primary outcomes were 30-day readmission rate, 30-day readmission due to sepsis, and 30-day mortality.
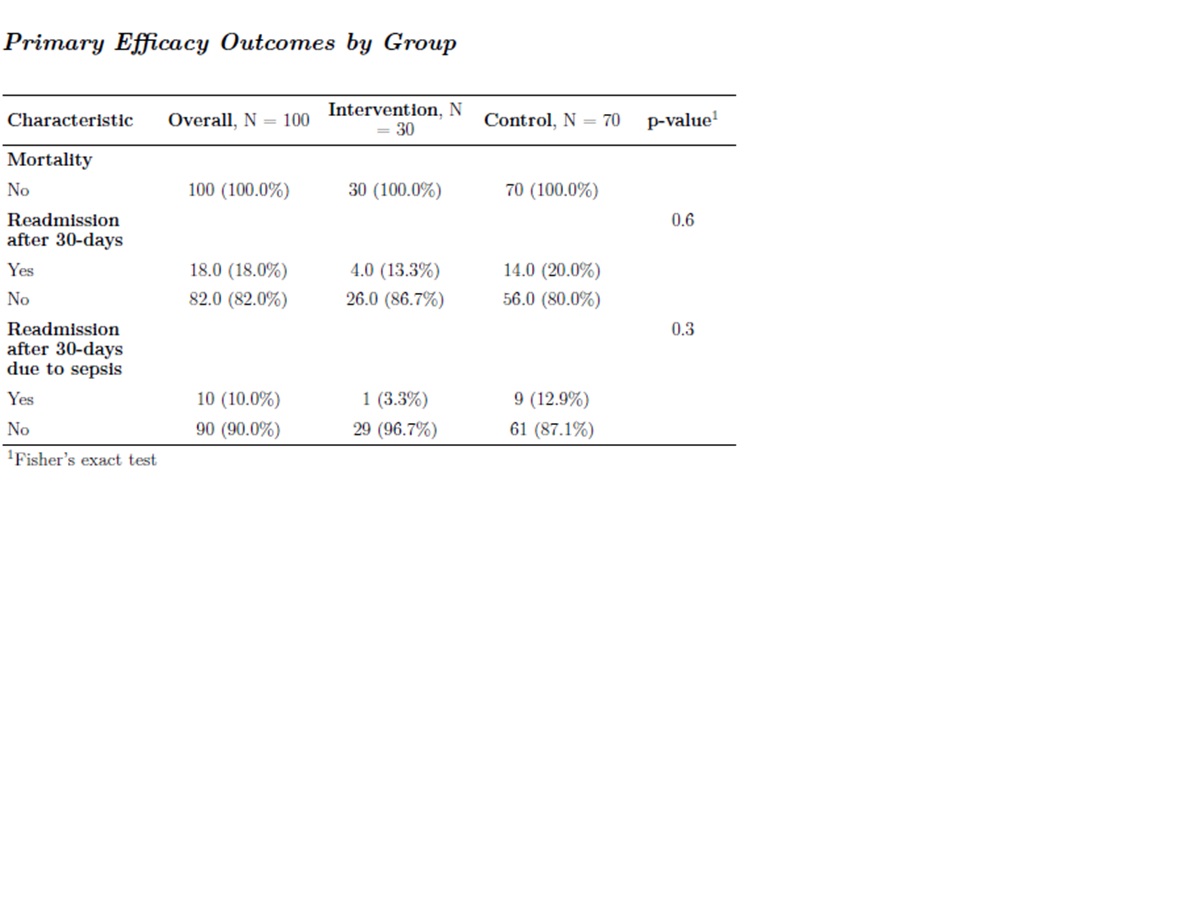
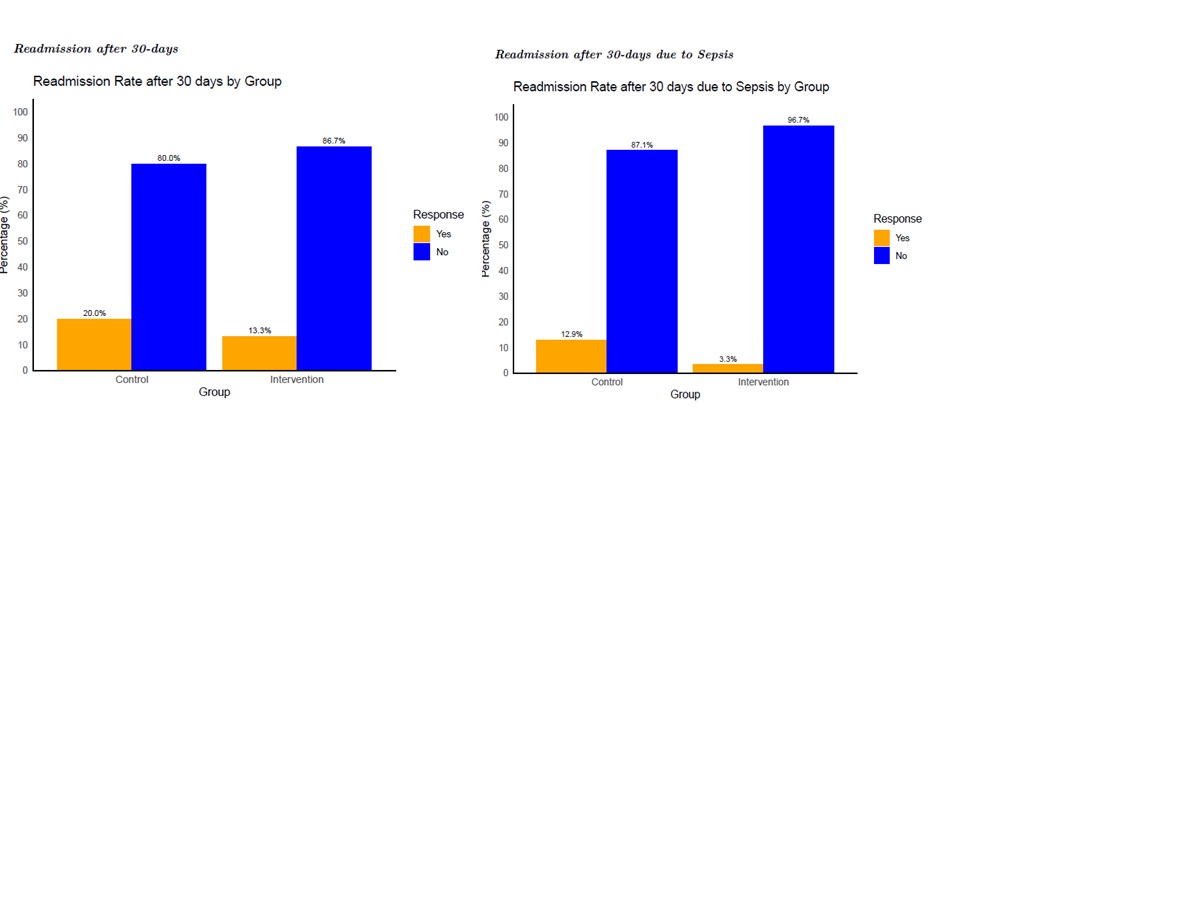
Results: From October 2022 to August 2023, 54 patients from the internal medicine services were consented and received the vital signs kit upon discharge. Of these, 30 patients (55%) completed at least one telehealth visit follow-up and were included in our intervention group. Among the 30 patients, ages ranged from 26 to 78 years, with an average of 54 years old and a standard deviation of 14.7. The gender distribution was similar, with males consisting of 47% and females consisting of 53%. Racially, 13% were African American, and 87% were White. In the intervention group, 4/30 patients (13%) of patients were readmitted within 30 days and no mortality events occurred. The distribution of the primary outcomes of the study: 30-day readmission, 30-day readmission due to sepsis and mortality, are presented in Table 1. While the difference in overall readmission rates was not statistically significant, readmission rates in the intervention group were lower (4/30 (13.3%) vs. 14/70 (20%) in the matched control group). There were no mortality events in the intervention and control groups. There was a difference in the readmissions due to sepsis, with only 1 out of 4 patients (25%) in the intervention group being readmitted due to sepsis compared to 9 out of 14 patients (64%) in the control group, although this difference was statistically significant.
Conclusions: This pilot program enrolled patients with sepsis who received a multicomponent post discharge program based on telehealth including vital signs kits. The intervention demonstrated lower readmission rates (13.3% vs. 20%) and fewer sepsis-related readmissions, though differences were not statistically significant. We were able to demonstrate that this strategy is feasible and economically viable. Future interventions should prioritize high risk patients through more intensive monitoring, such as additional follow-up visits.