Case Presentation: Milk alkali syndrome (MAS) was initially described in the early 1900s with the utilization of calcium alkali treatments for gastric ulcers and is characterized by the triad of hypercalcemia, metabolic alkalosis, and acute kidney injury (AKI). In modern times, it is usually secondary to calcium supplementation or excessive antacid consumption. Here, we describe a case of milk-alkali syndrome caused by excessive iatrogenic administration exacerbated by standard prescription.Description:A 60-year-old male with a history of recurrent laryngeal squamous cell carcinoma status post total laryngectomy, partial pharyngectomy and total glossectomy presented with two days of altered mental status and fevers. He was recently discharged from the hospital for the aforementioned surgical procedures and was started on a gastrostomy feeding. Initial serologies revealed severe metabolic alkalosis with a pH of 7.50, bicarbonate 38.3 mmol/L, serum calcium of 18.0 mg/d, and new severe AKI with creatinine increasing from 0.3 to 1.2 within a week. Later, a PTH of 2 pg/mL, 25-hydroxyvitamin D, and a PTH-related peptide within normal limits effectively ruled out other causes of hypercalcemia. At the previous hospitalization, due to mild hypocalcemia from acquired hypoparathyroidism, he was discharged with calcitriol and calcium-vitamin D supplements. His daily dose of calcium from tube feeds alone was 1.4g/day; however, including his supplements, his daily intake was approximately 6g, 5 times the recommended daily intake. The calcitriol likely also contributed to the rapid development of hypercalcemia. He was treated with aggressive IV fluids, calcitonin, and IV zoledronic acid, and the tube feed formulation was switched to one with lower calcium content. His mentation improved rapidly, and after 4 days, his calcium levels normalized, and renal function returned to baseline.
Discussion: The primary etiologies of symptomatic hypercalcemia in the hospital setting are primary hyperparathyroidism and malignancy; however, MAS is now responsible for more than 10% of cases and has become the third leading cause. Characterized by the triad of hypercalcemia, metabolic alkalosis, and acute kidney injury, MAS is a diagnosis of exclusion. In patients with known malignancy, it is easy to overlook MAS. More appropriately termed “calcium-alkali syndrome,” the modern MAS typically evolves after ingesting at least 4g elemental calcium/day; however, there have been reports of MAS with even 1-1.5g of supplementation, especially in high-risk individuals such as this patient (low body mass, chronic kidney disease, poor diet, and older age). Patients also develop hypophosphatemia rather than classic hyperphosphatemia, as milk contains high phosphate levels, leading to this finding.Like other causes of hypercalcemia, aggressive hydration is the cornerstone of treatment, with calcitonin/bisphosphonates being utilized if severe symptoms are present.
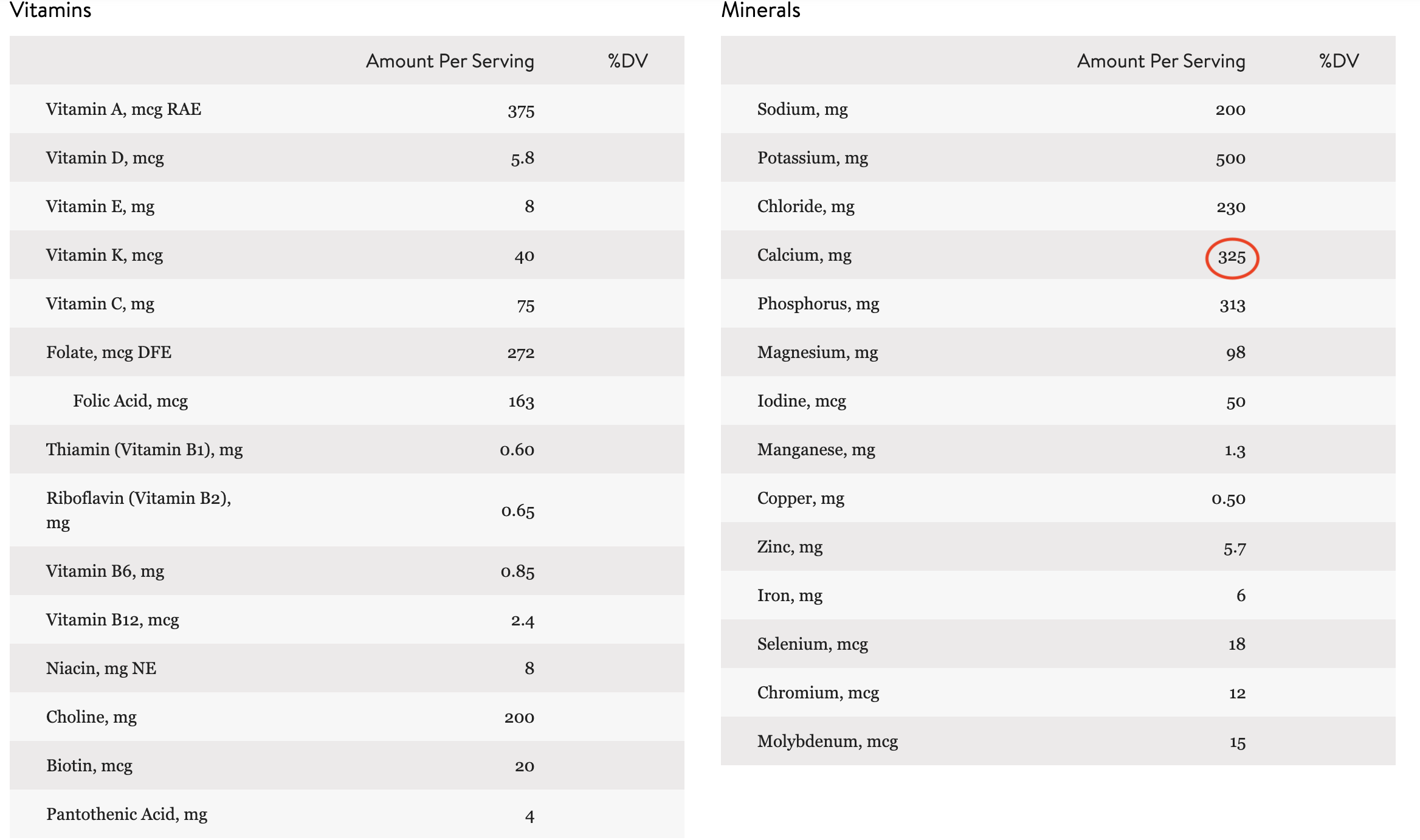
Conclusions: Tube feed formulations are commonly supplemented with vitamins and minerals, so additional supplementation is likely unnecessary and can lead to further iatrogenic complications. Adding additional supplements to gastrostomy-dependent patients needs to be considered carefully, as with dosing all other medications in context to their comorbidities to prevent adverse effects.