Background: Mortality risk assessment is crucial for predicting patient outcomes, assessing patient care delivery, and improving healthcare quality. Although high-quality medical documentation is critical for mortality risk assessment tools, provider documentation may be inconsistent, relies on coding teams for support, and may not directly reflect provider orders. Complete and precise documentation and coding can improve capturing patient complexity, predicting length of stay, and boosting hospital reimbursement. In January 2024, our academic medical center developed an electronic medical record (EMR) Smart Phrase called MiChart Clinical Assistance and Support Tool (MiCast), which automatically integrates 25 common mortality predictors into clinical documentation. We initiated a hospital medicine (HM) division quality improvement (QI) project in July 2024 to promote and increase the use of MiCast for improved mortality risk documentation.
Purpose: Evaluate the impact of a QI project on the percentage of EMR admission and progress note documentation using MiCast Smart Phrase, including the addition of mortality risk diagnoses across hospital medicine (HM) clinical services at a single academic medical center.
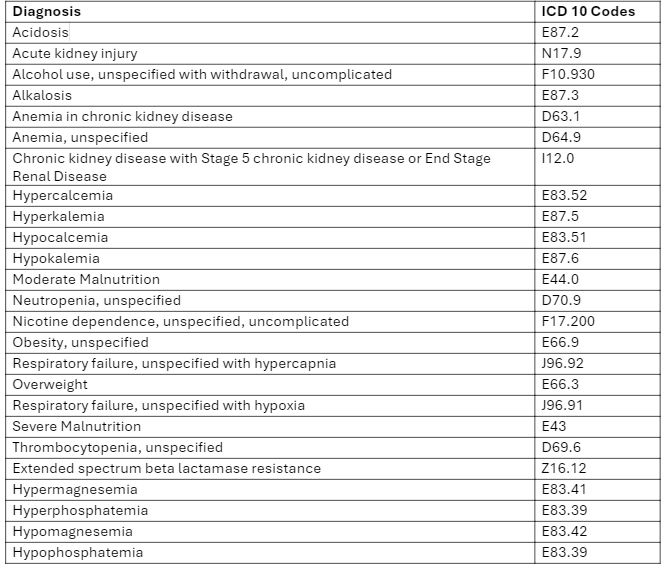
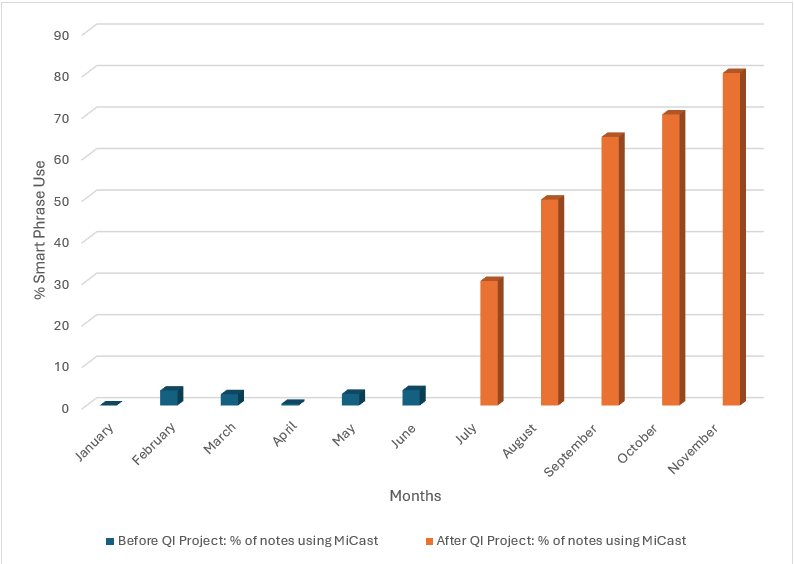
Description: The MiCast Smart Phrase targets 25 mortality risk diagnoses and related ICD-10 codes commonly found in inpatient settings (see Table), such as kidney disease, respiratory failure, blood disorders, electrolyte imbalances, malnutrition, and obesity. Content experts associated discrete test results and provider orders to each of the 25 listed clinical diagnoses. The MiCAST tool scans for those orders and test results and generates approved text in any note with the Smart Phrase. This text can include 0 to 25 new diagnoses. HM providers (physicians, physician assistants, nurse practitioners) review the generated text for accuracy, then sign and attest the note according to standard procedures. To better integrate the MiCast Smart Phrase into EMR documentation, we implemented several strategies: training sessions for HM physicians and advanced practice providers, creating a division dashboard to track MiCast adoption in clinical documentation and provide timely feedback, weekly chart reviews, email reminders to frontline providers, and monthly leadership meetings and progress updates. Our results (see Figure) show that before (January – June 2024) and during (July – November 2024) the QI project, MiCast was used in 2.2% (776/35,038) notes and 56.1% (15,269/27,207) notes, respectively. At least one additional mortality risk diagnosis was captured in 73.5% (11,788/16,045) of notes that included MiCast.
Conclusions: The introduction of a new EMR Smart Phrase, along with a comprehensive QI strategy, led to over 50% increase in MiCast Smart Phrase use in HM clinical notes at an academic medical center. This SmartPhrase was effective in capturing new mortality risk diagnoses to HM clinical documentation, given that nearly 75% of notes before and during the QI project added a mortality risk diagnosis.