Background: The under-reporting of adverse events has been a significant issue in patient and healthcare staff safety, and prevents improvement of individual and systemic errors in healthcare. As champions for quality and safety in their institutions, it is essential hospitalists who work with housestaff serve as role models to encourage trainees to report safety issues. Housestaff mainly receive patient safety training at orientation and through online modules. However, housestaff are often unable to recall details of this training (1) and perceive that reporting could lead to damage to personal and professional relationships (2).
Purpose: We developed a peer-to-peer workshop designed to transform attitudes, improve competencies, and decrease barriers to adverse event reporting by trainees at a university-affiliated academic medical center. The workshop was designed and presented by a resident interested in patient safety, with hospitalist oversight. The curriculum consisted of the following components: 1) a teaching case with a sample adverse event; 2) discussion of barriers to adverse event reporting; 3) information on how reports are triaged; 4) solutions to improve reporting rates; 5) instruction and sample submission of an adverse event report; and 6) examples of how reporting has led to systems changes. A survey was administered to assess pre and post-workshop attitudes, competencies, and knowledge of adverse event reporting. Preliminary data was analyzed with Microsoft Excel using paired t-test analysis.
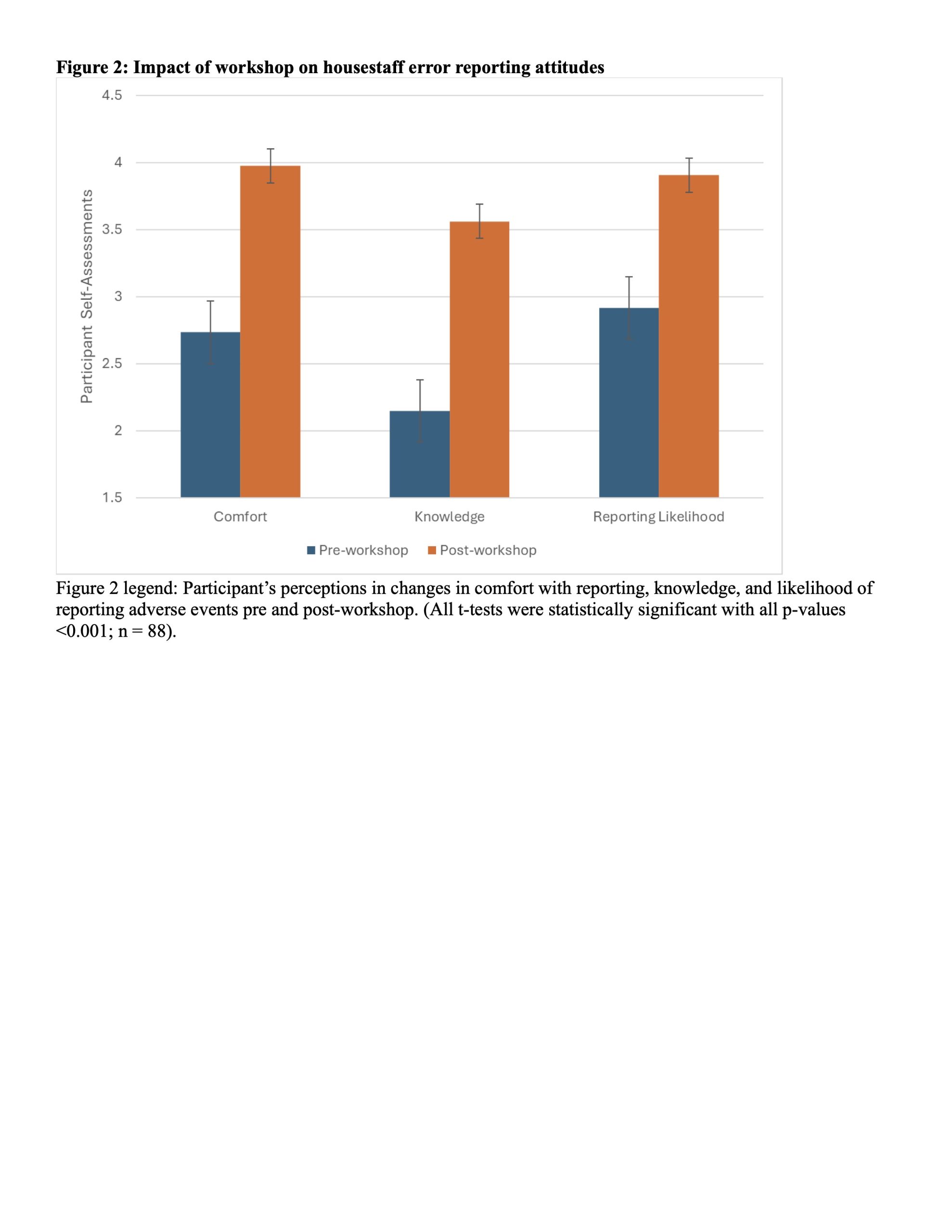
Description: Amongst 105 housestaff who participated in the workshop, ranging from PGY-1 to PGY-7, 67% reported never having submitted an adverse event report. While 58% of housestaff pre-workshop reported being exposed to an adverse event and 29% of housestaff unsure if they have been exposed, 70% of participants post-workshop describe witnessing an adverse event with 15% of participants unsure. Perceived barriers to reporting are detailed in Figure 1, with being too busy (76%) as the most common. Workshop participants reported significant improvements in their comfort level, knowledge, and likelihood to report adverse events following the workshop, as demonstrated in Figure 2. Approximately 92% of participants found the workshop at least moderately useful, and 90% of participants thought the workshop decreased their barriers to event reporting.
Conclusions: A peer-to-peer workshop can improve comfort, knowledge, and likelihood of reporting adverse events among physician trainees. We identified key barriers to event reporting and demonstrated that interactive workshops can help reduce these barriers. Academic hospitalists should consider support of housestaff peer training initiatives. Next steps include exploring the long-term impacts of this workshop.