Background: Diagnostic errors (DE) are common in hospitalized patients, especially those with an unintended escalation of care, and cause substantial harm. However, individual hospitals currently lack methods to analyze local diagnostic process failure patterns to identify targets for quality improvement efforts.
Purpose: The AHRQ funded UPSIDE study identified key diagnostic process failures across a national hospital network using the Diagnostic Error Evaluation and Research (DEER) taxonomy. We employed a systems engineering approach combining heat map analyses and Pareto diagrams based on UPSIDE data to identify site-specific diagnostic process failures. By benchmarking local variation in process failures against system-level data, individual hospitals could customize local diagnostic safety improvement efforts.
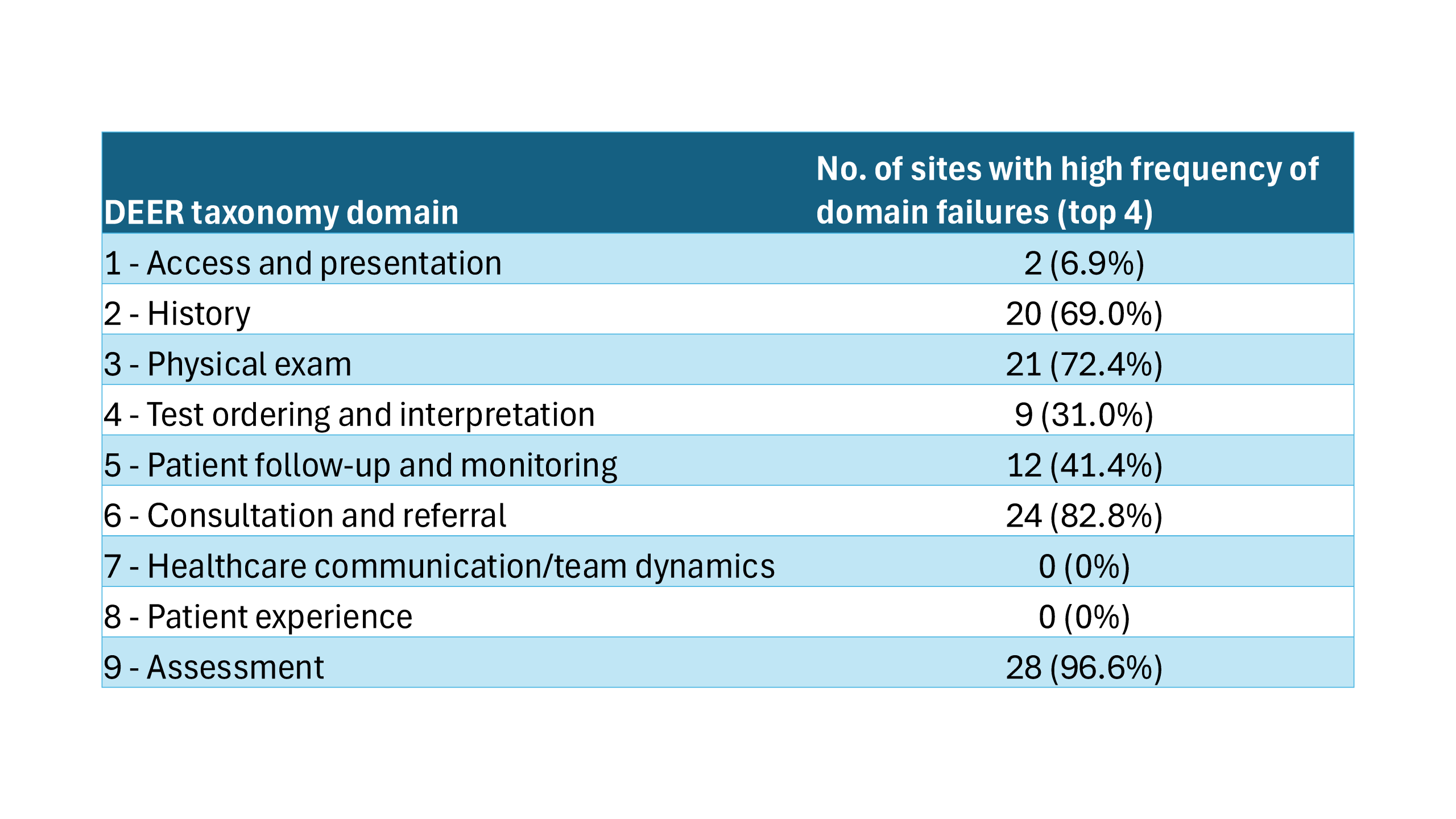
Description: Using UPSIDE data, we developed a standardized analytical approach to characterize diagnostic process failures at both system and site levels. We analyzed cases with confirmed diagnostic errors at 29 hospital sites across each DEER taxonomy domain. After normalizing the data between sites, we created heat maps to visualize the distribution of failures across domains from weighted samples of analyzed cases from each site (Figure). We then utilized Pareto diagrams to identify the categories accounting for the most frequent errors (Figure). At the system level, key process failures were in the domains of assessment (6,781 weighted events), test ordering/interpretation (6,083), history-taking (5,432), and patient monitoring (3,520). Site-level analyses revealed that while assessment problems were consistently prominent across sites (present in the top 4 domains of 97% of sites), other domains showed substantial variation (Table). For example, test ordering/interpretation, while highly represented in the overall cohort, was present in the top 4 process failure domains in only 9 (31%) sites.
Conclusions: Our systems engineering approach provides hospitals with a practical methodology to analyze their diagnostic error patterns, identify site-specific variation, and prioritize improvement efforts. By identifying diagnostic process faults specific to their site, this methodology enables hospitals to benchmark against system-level data, informing targeted intervention development. Future work will evaluate the effectiveness of targeted interventions based on this analysis.