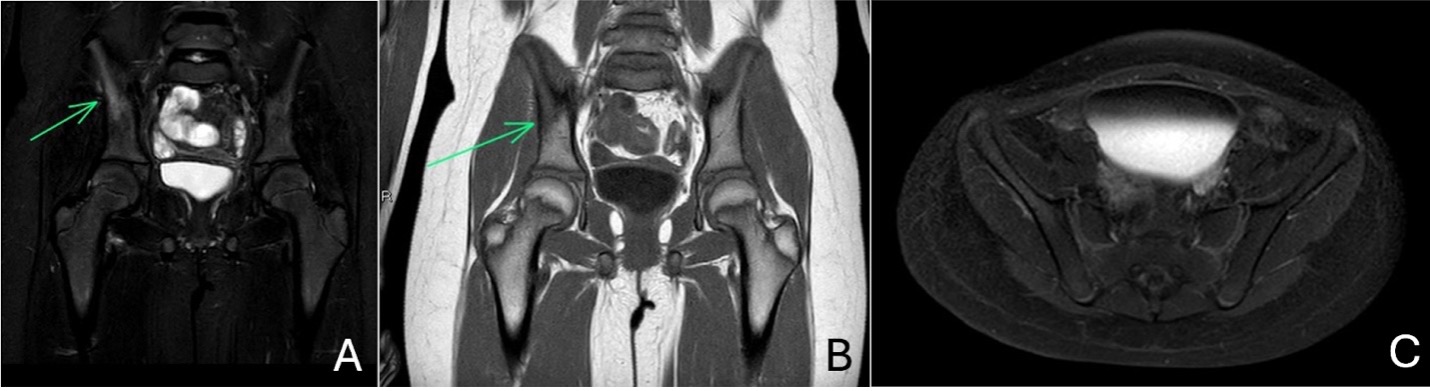
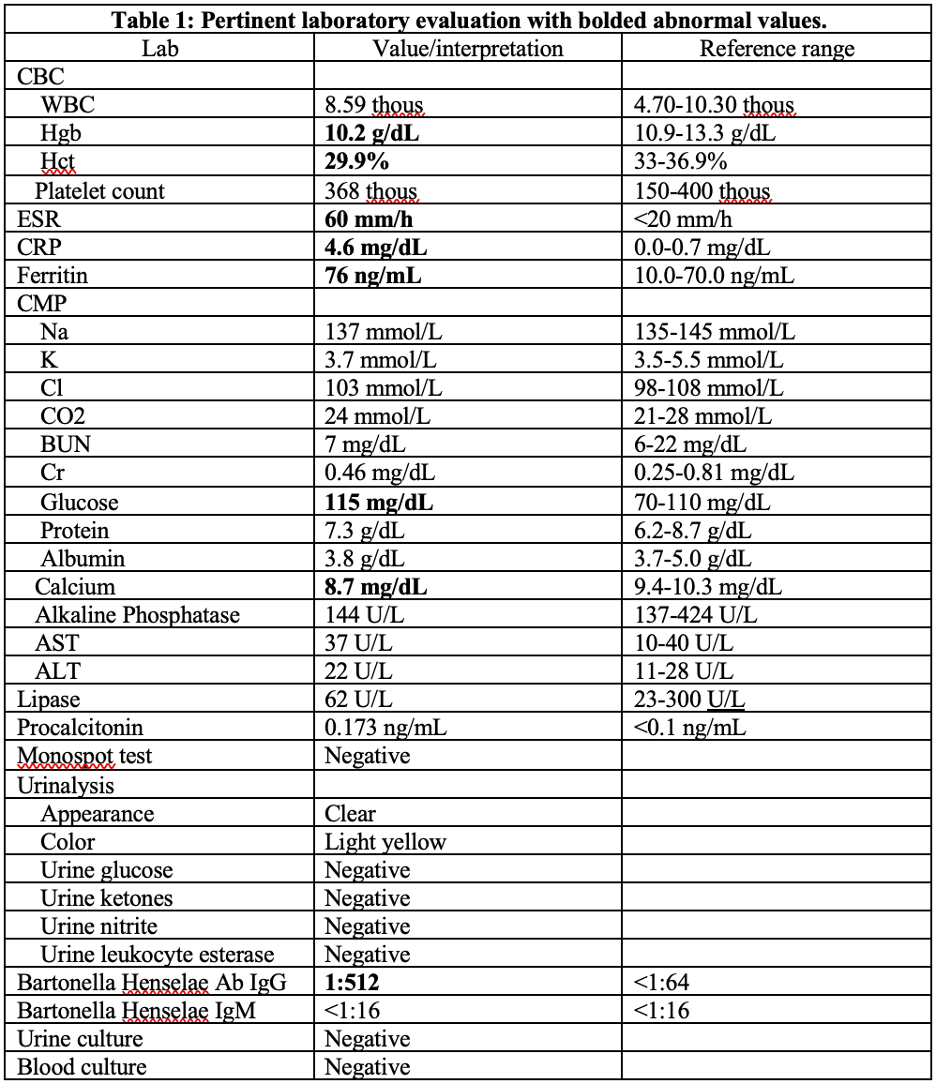
Case Presentation: A previously healthy, vaccinated 9-year-old female on amoxicillin for recent Group A strep pharyngitis presented to the emergency department with a 10 day history of daily fevers and severe right lower quadrant abdominal pain limiting her ambulation and activity level. She denied any headaches, nausea, vomiting, hip pain, knee pain, or traumatic injuries. Social history notable for recent travel to Texas as well as exposure to two dogs in the home and a cat that ran away but returns when they leave food out.Upon initial exam, she was febrile, with tachycardia and tachypnea for age. Abdominal exam revealed tenderness to palpation in both right and left lower quadrants. She had no pain with full range of motion in her bilateral hips, without overlying erythema or edema. No axillary or inguinal lymphadenopathy appreciated. Exam was otherwise unremarkable.Laboratory evaluation most notable for an elevated CRP, ESR, and ferritin (Table 1). Presentation initially concerning for appendicitis although unable to visualize appendix on ultrasound. Subsequent MRI of appendix without evidence of appendicitis, however did reveal marrow edema consistent with right ileum osteomyelitis that was later confirmed with a dedicated MRI of her right hip and pelvis (Figure 1). The patient was started on IV cefazolin and, after consultation with our Pediatric Infectious Disease team, Bartonella serologies were added to ongoing workup. Abdominal pain improved with antibiotics and aggressive bowel regimen. Inflammatory markers normalized and the patient’s fever defervesced prior to discharge. Bartonella titers returned positive, 1:512, indicating final diagnosis of Bartonella henselae osteomyelitis. She was discharged on oral cephalexin for a total of 5 weeks of antibiotic therapy. She is doing well upon follow up with no residual pain.
Discussion: Bartonella henselae infection, or cat-scratch disease, most commonly presents as regional lymphadenopathy. Complicated, or atypical cat-scratch disease develops in 5-14% of immunocompetent patients and may reflect bloodborne disseminated disease in almost any organ system.Bartonella henselae infections are most common in children 5-9 years old and best diagnosed with serology. Antibiotics are not required for localized cat-scratch disease but are usually considered in immunocompromised and acutely ill immunocompetent patients with systemic symptoms such as our patient with osteomyelitis. Multiple antimicrobial agents have demonstrated effectiveness against bartonella, including beta lactams, as was our treatment of choice.
Conclusions: Bartonella henselae osteomyelitis is an uncommon cause of pediatric osteomyelitis, but important to include on the differential when considering osteomyelitis of unclear origin. Even with careful history taking, history may be negative for classic cat scratch exposure, therefore it is important to maintain a high index of suspicion, as vague symptoms and poorly localized pain may delay diagnosis. Early detection and appropriate treatment are important to prevent chronic infection, avascular necrosis, or growth abnormalities.