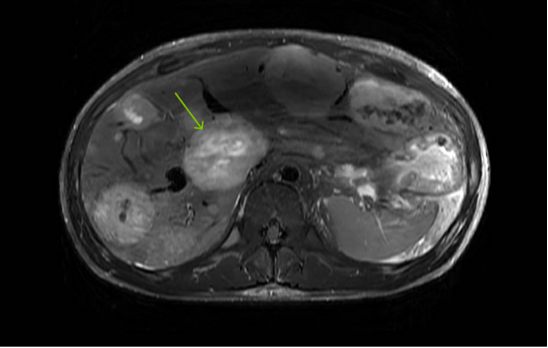
Case Presentation: A 21-year-old male with no prior medical history presented with progressive dyspnea and bilateral lower extremity edema that began four months prior. On exam, he had JVD to the mandible, positive hepatojugular reflux, a harsh grade III/VI systolic murmur at the right lower sternal border, pitting edema to the hips, and an erythematous rash on the chest, face, and upper extremities. The patient also reported four years of diarrhea.Routine blood tests indicated alkaline phosphatase of 226 IU/L, BNP of 173 pg/mL, and unremarkable troponin and TSH levels. EKG revealed sinus tachycardia with right axis deviation and incomplete right bundle branch block. Transthoracic echocardiogram (TTE) showed severe tricuspid regurgitation due to leaflet malcoaptation (Figure 1).CT chest angiography, negative for pulmonary embolism, incidentally identified multiple hepatic masses. MRI of the abdomen demonstrated diffuse hepatic metastatic disease with mesenteric lymphadenopathy (Figure 2).The patient’s clinical presentation and imaging findings, alongside a 24-hour urinary excretion of 5-HIAA of 444.3 mg/24 hours, led to the diagnosis of carcinoid heart disease. Liver biopsy confirmed a well-differentiated neuroendocrine tumor, grade 1.Initial treatment focused on symptom management. Intravenous diuretics improved dyspnea and edema, and octreotide alleviated cutaneous flushing and diarrhea. He was discharged on oral diuretics and octreotide with outpatient oncology follow-up for chemotherapy discussions and a referral to cardiothoracic surgery for tricuspid valve replacement.
Discussion: CS is a paraneoplastic syndrome associated with neuroendocrine tumors (NETs), occurring in 30-40% of NET patients. (1) Most primary tumors originate in the GI tract, releasing hormones that undergo hepatic metabolism to 5-hydroxyindoleacetic acid (5-HIAA) for urinary excretion. (2) Systemic effects arise when liver metastasis bypasses this metabolism, leading to fibrous tissue deposition on right-sided heart valves, causing dysfunction. (3) CHD typically affects individuals aged 50-70. (4) As survival improves, CS complications like CHD are seen more frequently. (5) CHD is often diagnosed late, with only 20% of CS patients initially presenting with it. (6)Patients with CHD often demonstrate gradual symptom progression. (8) In this case, the patient presented with features of heart failure, and given his young age, CS was not immediately considered. Clinicians should maintain a high index of suspicion for CS in young patients presenting with RHF alongside other systemic symptoms. Diagnostic tools such as CT abdomen/pelvis, 24-hour urine 5-HIAA, and TTE/TEE should be utilized when clinical suspicion arises.
Conclusions: This case of carcinoid heart disease in a young patient highlights the diagnostic challenges in identifying CHD, particularly in the absence of classic risk factors. Clinicians must maintain a broad differential diagnosis and consider uncommon etiologies such as CS when managing young patients with RHF. We aim to contribute to the limited literature on CS in young patients, with hopes of raising clinician awareness when evaluating RHF in this population.