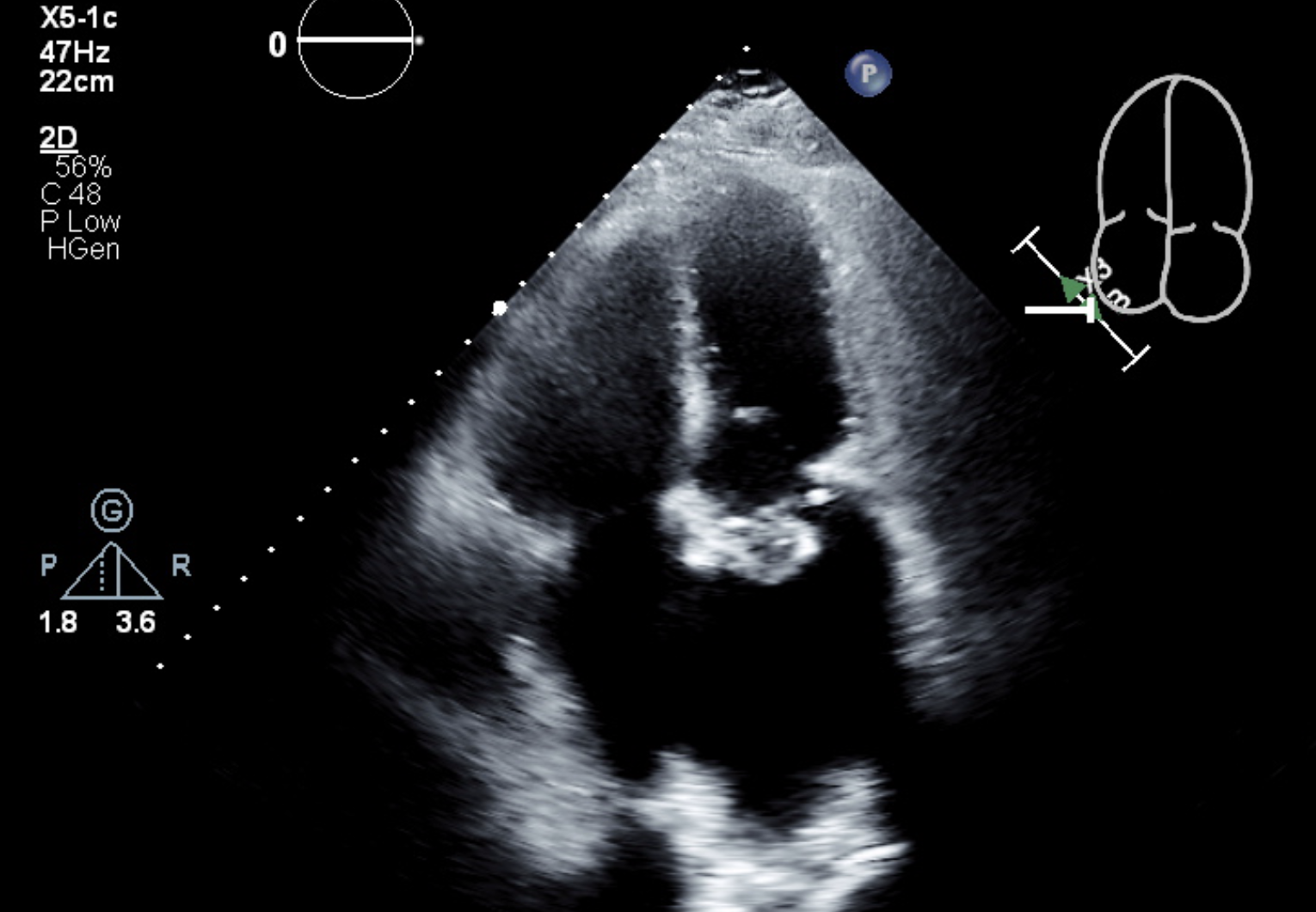
Case Presentation: A 66-year-old male with a history of neuromyelitis optica (NMO) on rituximab, paraplegia, knee arthroplasty with prior prosthetic joint infections, and chronic urinary catheter complicated by frequent UTI’s with prior growth of Pseudomonas, methicillin-resistant S. aureus (MRSA), E. coli, and Proteus, presented with fever and purulent urine. He was insensate below the umbilicus and so unable to report dysuria. On admission he was febrile to 103° F and workup revealed leukocytosis of 27,000, pyuria, and bacteriuria. Chest x-ray revealed nonspecific opacities possibly suggesting infection. Given concern for immunosuppression and culture history, he was started on empiric meropenem and vancomycin. Blood cultures grew MRSA at eight hours, but urine culture grew only pseudomonas raising questions as to the source of bacteremia. Further examination revealed erythema and drainage at his left knee arthroplasty scar reportedly ongoing for months. Chart review revealed multiple prior knee infections with positive cultures for both pseudomonas and MRSA. Orthopedics was consulted for knee aspiration to reassess the source of infection, but the procedure was unsuccessful. He was planned for outpatient hardware removal for presumed chronic prosthetic joint infection. On day five, a medical student noted the patient had slurred speech and left-sided weakness. Imaging revealed left subarachnoid hemorrhage and bilateral scattered infarcts. He was not a candidate for stroke intervention. A recently ordered echocardiogram subsequently demonstrated a 4.2 cm mitral valve vegetation. Cardiac surgery was consulted but deemed him not a surgical candidate given cerebral hemorrhage. Neurosurgery was consulted with plan for angiogram for possible mycotic aneurysm. However, the patient transitioned to comfort measures given his decline and low likelihood of recovery. He expired shortly after.
Discussion: This case demonstrates the danger of anchoring bias in complex patients. Our patient’s known UTI’s led to early diagnostic closure, and when contradicted by culture data, attention was turned toward possible joint infection. It was not until he suffered a catastrophic neurological complication that the diagnosis of IE was seriously considered. Treatment of IE is also challenging. Our patient sustained likely cardioembolic stroke despite early antimicrobial treatment. Guidelines suggest early surgery for large vegetations (>10 mm) and left-sided S. aureus IE, but our patient was unfortunately deemed a poor surgical candidate. It should be noted our institution does have a multidisciplinary endocarditis team (MDET) which has been shown to reduce mortality of IE. Our patient unfortunately deteriorated prior to discussion with the MDET, suggesting opportunity for further systemic optimization in the approach to IE.
Conclusions: Even in chronically infected patients, IE must be considered early in the differential.