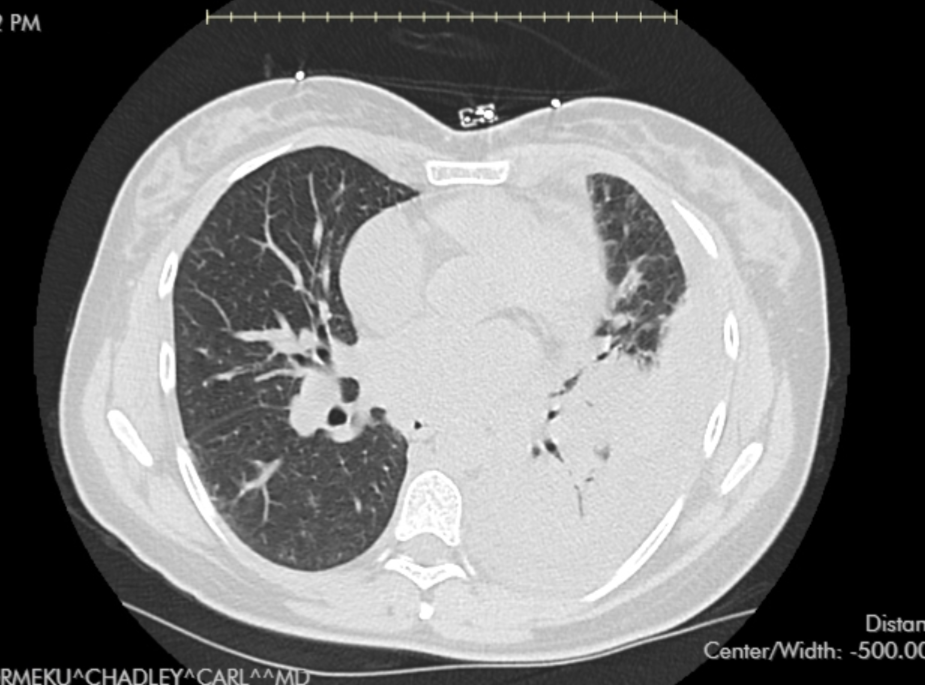
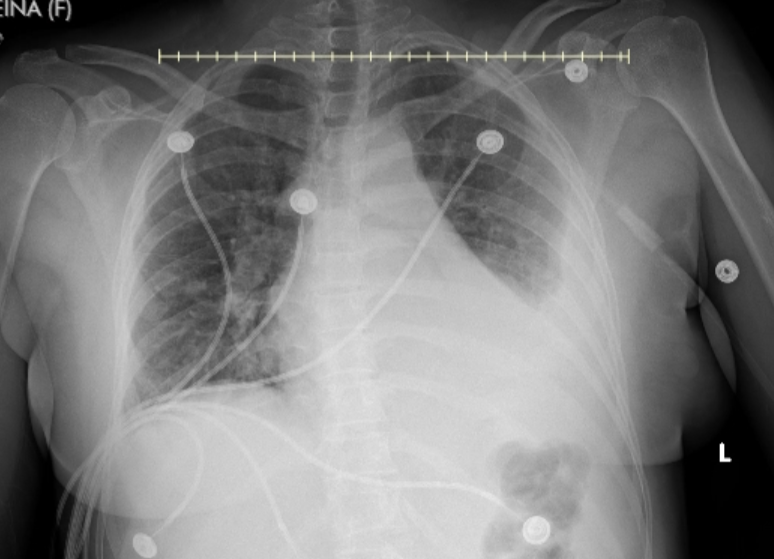
Case Presentation: A 39-year-old Hispanic female, with no significant past medical history presented with complaints of fever, chills, myalgia, and cough ongoing for the past 10 days. The patient had a heart rate of 143 beats per minute, a Temperature of 103.4° F, and a respiratory rate of 33. The patient had a WBC count of 33000 cells/L, hemoglobin of 9.9 g/dl, and platelet count of 395000 cells/L. Chest CT scan showed moderate-to-large loculated left-sided pleural effusion with scattered infiltrates on the right lung lobe. Mycoplasma pneumonia PCR was positive in the blood and in the pleural fluid after thoracentesis. Extensive work-ups done were negative for other pathogens including respiratory Viral panel, MRSA, pneumococcal antigen, and blood culture. The serum mycoplasma IgM level was 1.06U/L (1006 Units/ml). Ultrasound-guided chest tube placement was performed, and analysis of the pleural fluid was suggestive of empyema. The bacterial culture of pleural fluid was negative. Also, Pleural fluid mycoplasma IgM was 4.05 U/L(4005 Units/ml). The patient was empirically treated with vancomycin, and meropenem, and later switched to and discharged on Levofloxacin for a total duration of 2 weeks. The patient also received tissue plasminogen activator and Dornase and the patient had remarkable clinical improvement.
Discussion: Mycoplasma pneumoniae is a frequent cause of community-acquired pneumonia, especially in younger populations. Typically, the clinical course of Mycoplasma pneumonia is mild, with patients often experiencing symptoms such as low-grade fever, cough, and malaise. Hospitalization is generally not required unless there are significant comorbidities or complications. Empyema, is an exceedingly rare complication of Mycoplasma pneumonia, with only a few cases reported in adults.The diagnosis of Mycoplasma pneumonia often relies on clinical features and supportive laboratory findings, such as elevated serum IgM levels, which in this case exceeded 1,000 U/mL. PCR testing is a valuable tool for confirming the presence of Mycoplasma pneumoniae in both blood and pleural fluid. In this case report, the absence of other pathogens in the pleural fluid culture, along with the positive Mycoplasma PCR, strongly suggests that Mycoplasma pneumoniae was the primary pathogen responsible for this infection.The treatment of Mycoplasma pneumonia typically involves macrolides or fluoroquinolones, with a course lasting 7-14 days. However, in cases complicated by empyema, broader antibiotic coverage may be warranted initially, as was done in this case. Prompt drainage of the empyema is crucial for reducing the bacterial load, alleviating symptoms, and preventing mortality and morbidity. The use of intrapleural fibrinolytic therapy has been shown to enhance drainage in complex pleural effusions and empyemas, as seen in this case report.
Conclusions: This case highlights the importance of considering Mycoplasma pneumoniae as a causative agent even in complicated pneumonia and empyema. Early identification of the causative organism and appropriate management, including antibiotic therapy and drainage of the empyema, are essential for optimizing patient outcomes. Clinicians should remain vigilant for atypical presentations of common infections, particularly in otherwise healthy individuals who develop severe complications. This case also emphasizes the utility of advanced diagnostic techniques such as PCR in identifying uncommon pathogens and guiding targeted therapy.