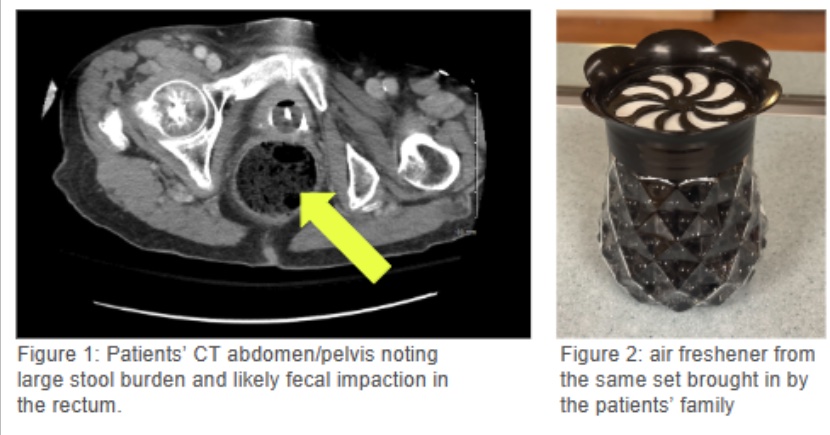
Case Presentation: The patient was an 85-year-old female who presented to the hospital with encephalopathy, rigors, new onset atrial fibrillation with rapid ventricular response and shock. Her past medical history was only noted as dementia and hypertension. Due to her change in mental status, CT head and CTA head and neck were obtained which did not note any signs concerning for stroke. On presentation her BP was 59/42, with lactic acidosis to 2.2, potassium 2.6 and temperature of 88 degrees Fahrenheit. She was admitted to the ICU and treated for presumed sepsis, including full 30 cc/kg fluid bolus, vancomycin, piperacillin-tazobactam and norepinephrine to maintain MAP >65 mmHg. The atrial fibrillation and lactic acidosis resolved following fluid resuscitation and hypokalemia corrected promptly with replacement. External warming measures led to a resolution of hypothermia. Her mental status also improved to baseline. Evaluation was unable to find any source of infection or alternative cause for encephalopathy; including no growth on blood cultures, unremarkable UA, no infiltrates on CXR, and no concerning findings on CT chest/abd/pelvis. Imaging incidentally noted constipation and possible fecal impaction. During enema, nursing staff noted unusual appearance to her stool including paper products, fabric and what appeared to be beads. Collateral history was obtained from the patients’ daughter, and it was determined that these were likely air freshener beads that had recently disappeared from the home bathroom. The brand was identified, and poison control was called, and the brand determined the most likely relevant ingredient was isopropyl alcohol; they did not make any further recommendations but instructed further supportive care. She had no known history or active suicidal ideation, hallucinations, delusions or previous toxic ingestion. Following supportive measures her mental status returned to baseline, and she was discharged to skilled nursing facility.
Discussion: Adults over the age of 75 are the smallest demographic that contact poison control for toxic ingestion; however, toxic ingestions in this demographic can be catastrophic due to altered metabolism and comorbid conditions. Toxic ingestion of air freshener products is not well documented in the literature; however, isopropyl alcohol is the active ingredient in products like rubbing alcohol and hand sanitizing products. Typical presentation of isopropyl alcohol toxicity is a rapid toxic encephalopathy followed by depression of the central nervous system. Its distribution can also lead to inhibited respiratory drive, peripheral vasodilation and decreased cardiac inotropy which can lead to shock and respiratory failure in severe cases. Patients will present typically with a ketosis without acidosis and an elevated osmolar gap; if available, an isopropanol level above 500 mg/L is suggestive of toxicity. In cases of severe poisoning, hemodialysis can be considered; however, there is limited data demonstrating significant clinical benefit in comparison to supportive care.
Conclusions: In cases of encephalopathy and undifferentiated shock, Ingestion of toxic alcohols should be considered. Evaluation should include an osmolar gap, and if relevant this should be followed up with specific tests such as an isopropanol level. There is limited data on the superiority of dialysis over supportive care in isopropyl alcohol toxicity, but it can be considered in cases of severe poisoning.