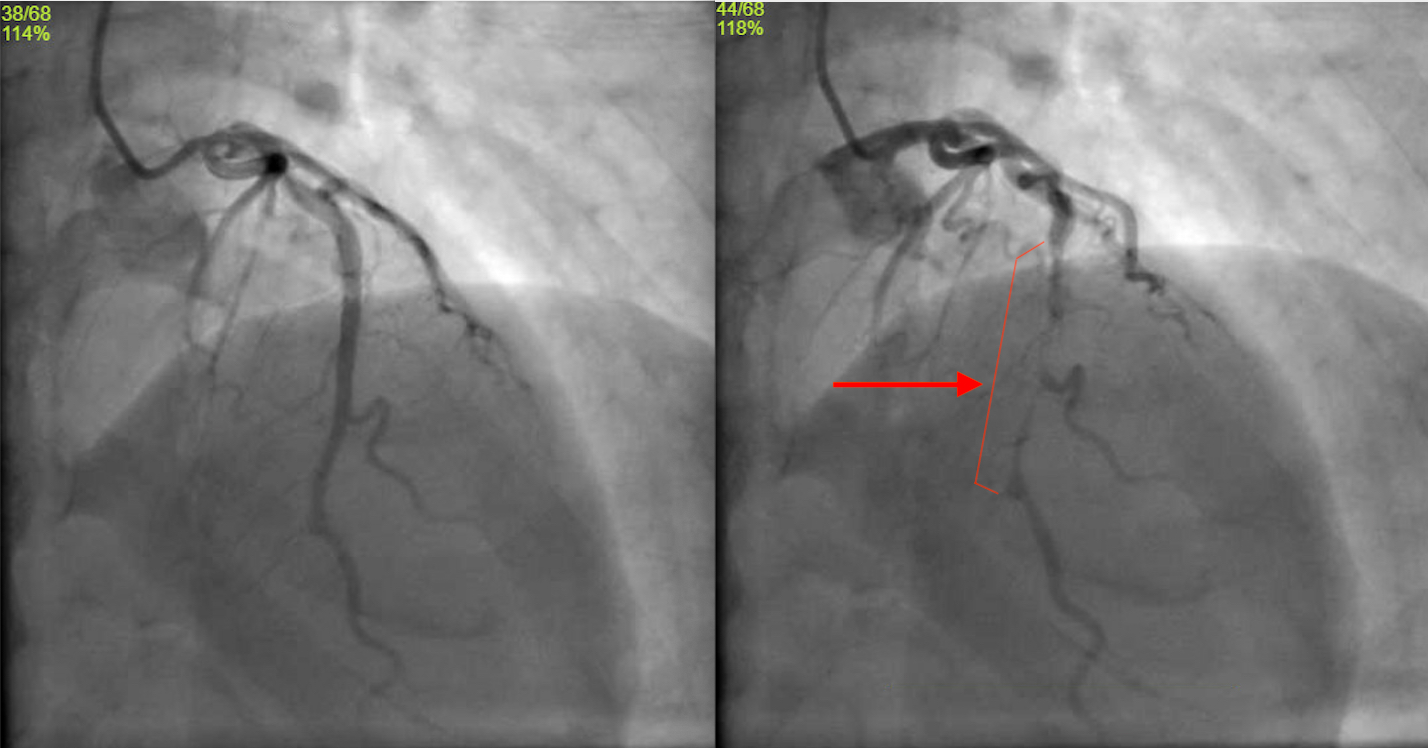
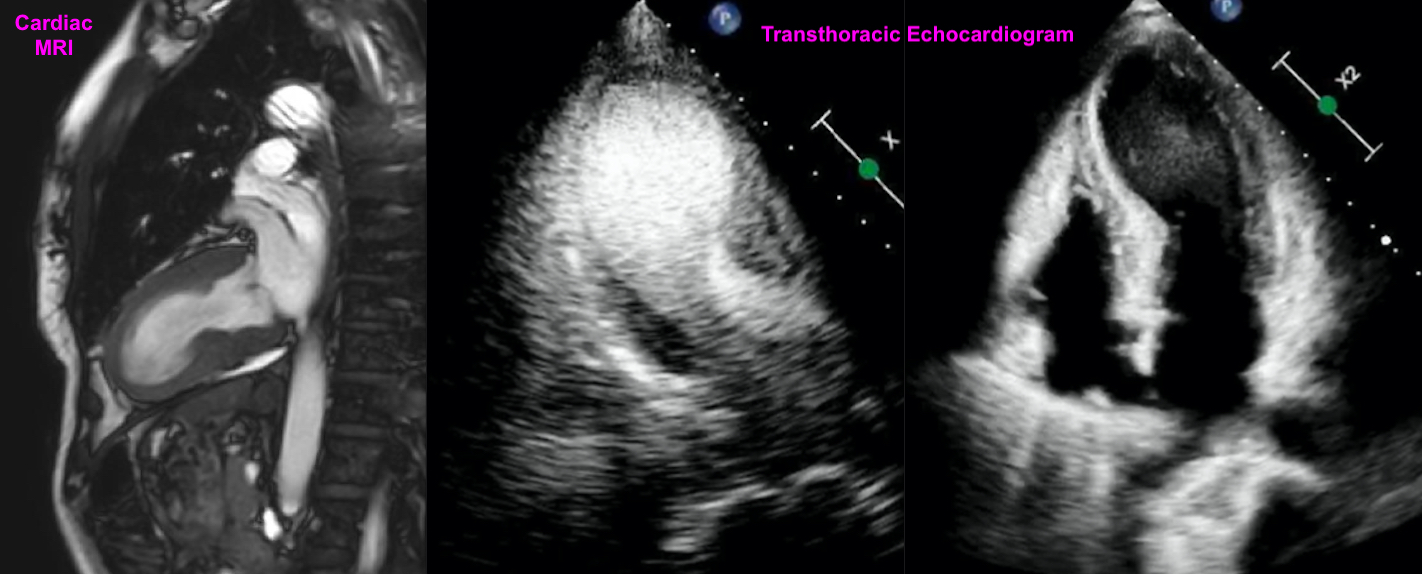
Case Presentation: A 48-year-old female with Hashimoto’s thyroiditis (on Synthroid), prediabetes, and active tobacco use (30 pack-years) who exercises daily presented to the ER with chest pain after a high-intensity workout. The pain radiated to her left arm and neck and intensified to 10/10, associated with palpitations.On exam, she had cool extremities and diaphoresis. Vital signs: BP 93/63, Pulse 87, Temp 36°C, RR 17. An EKG revealed ST elevations in V3-V6 and II, III, aVF. Initial troponin was 696, rising to 1,641 and 2,458. CPK 564, CKMB 9.0. Coronary angiography showed no obstructive coronary artery disease but identified a large myocardial bridge (MB). Transthoracic echocardiogram (TTE) revealed an EF of 15-20%, apical akinesis, apical ballooning consistent with Takotsubo cardiomyopathy (TC), systolic anterior motion of the mitral valve, LV outflow tract gradient of 30-40 mmHg, and an apical LV mural thrombus.Her course was complicated by worsening hemodynamic instability, requiring inotropic support, phenylephrine and esmolol drips. She was weaned off these medications and discharged on metoprolol and anticoagulation for the LV thrombus. She was started on guideline-directed medical therapy (GDMT) for TC.Three days post-discharge, a cardiac MRI showed EF improved to 40%. Repeat TTE two weeks later showed EF of 60% with no wall motion abnormalities. At three months, MRI showed EF of 67% and resolution of the LV thrombus and Takotsubo morphology. The patient quit smoking, adopted a healthy diet, and showed further improvement with optimization of GDMT.
Discussion: A myocardial bridge (MB) is when a coronary artery dives into the cardiac muscle rather than lying above it. Once considered a benign anatomical variant, MB can have serious and potentially fatal consequences, even in patients without traditional cardiac risk factors. MB is often asymptomatic and may only be detected during cardiac catheterization or autopsy, with an estimated prevalence anywhere from 5-15%. Its severity correlates with the depth of vessel involvement within the muscle [6]. Management of MB remains under-researched, but medical therapy typically involves calcium channel blockers for vasospasm and beta blockers to reduce heart rate, contractility, and artery compression, while increasing diastolic filling time [1] [2]. Nitrates should be avoided, as they may exacerbate artery compression by vasodilating adjacent coronary segments [3]. For severe MB, percutaneous coronary intervention is an option, though carries risks like stent fracture, thrombosis, and perforation due to the anatomical compression from the bridge [4]. Coronary artery bypass graft or surgical myotomy may be required in extreme cases [5].The relationship between MB and TC requires more exploration. MB may contribute to TC, particularly with involvement of the left anterior descending artery. Compression during ventricular systole may trigger ischemia, contributing to TC [8] by causing LV hypokinesis, leading to blood pooling and LV elongation [9]. Multimodality imaging techniques can help elucidate the interactions between MB, spontaneous coronary artery dissection, and TC [10] [11].
Conclusions: This case underscores the importance of considering MB in differential diagnoses, as well as understanding its medical management. Further research is necessary to clarify the relationship between MB and TC, which may lead to more effective management strategies and outcomes.