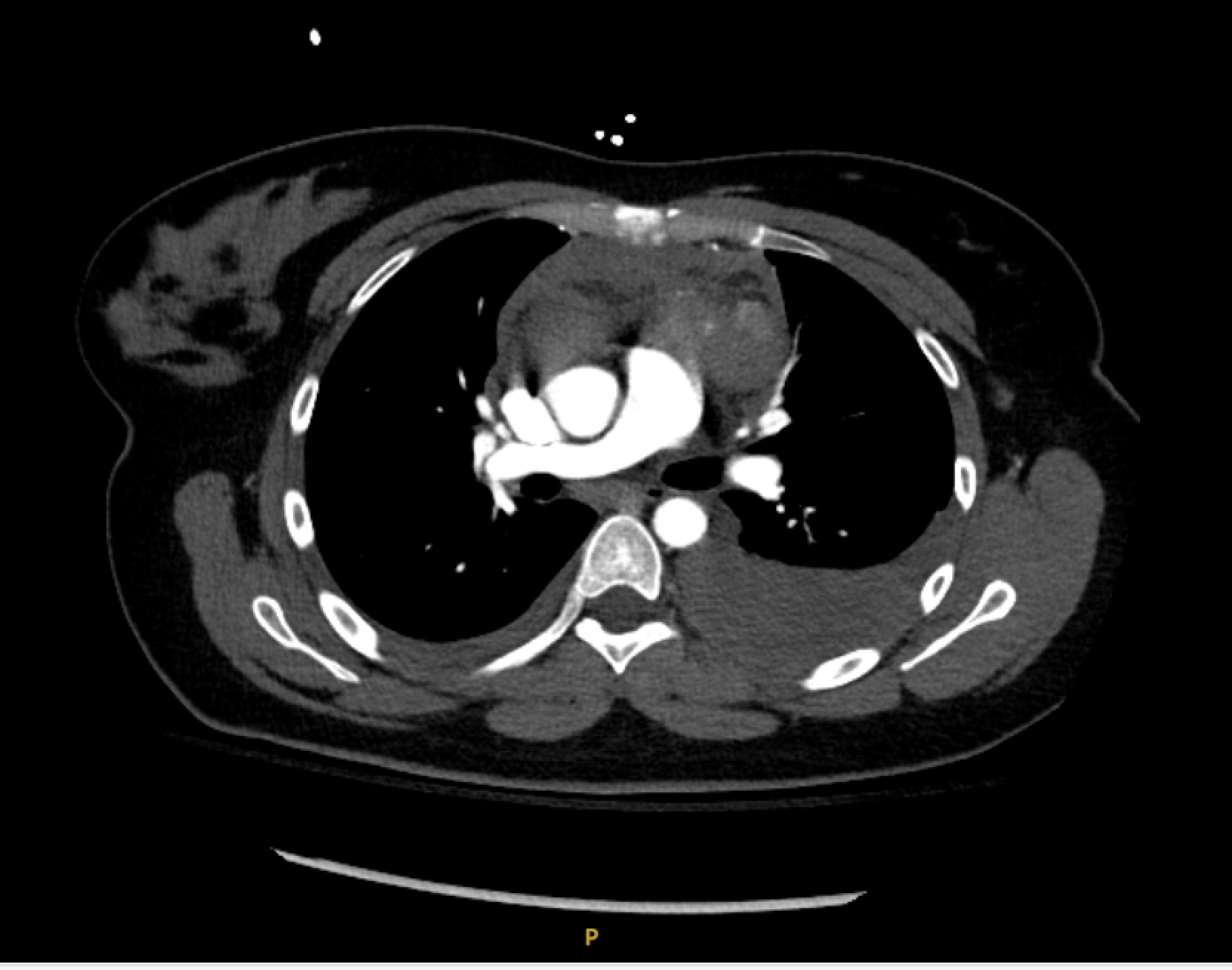
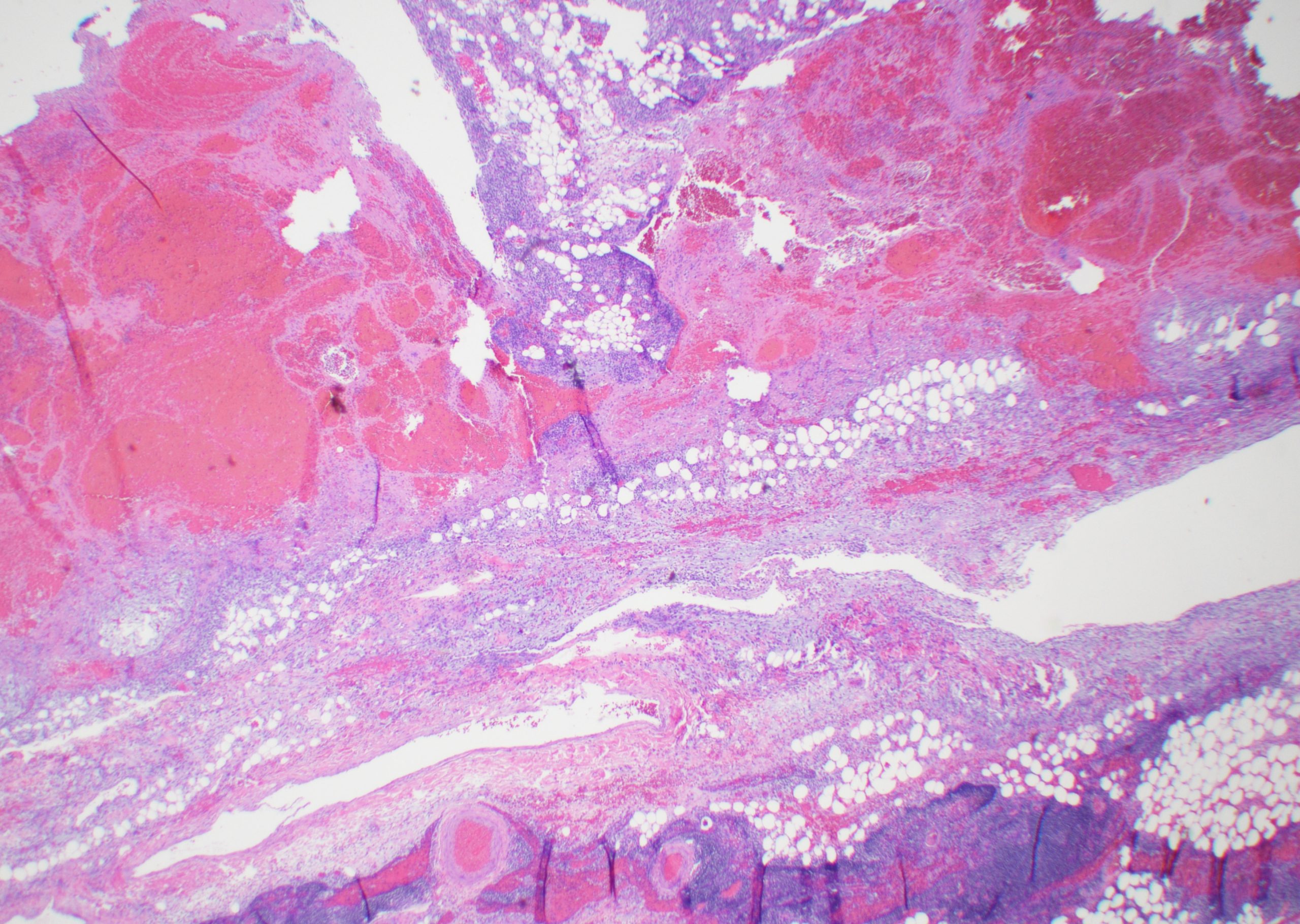
Case Presentation: The patient is a 32-year-old female who presented with a five week history of chest pain that radiated to the left shoulder and back with associated chest wall bruising that resolved prior to presentation. Pain was 7/10 in intensity, worsened with deep inspiration, positional, and associated with mild dyspnea. Medical history includes rheumatoid arthritis, and preeclampsia. On presentation, vital signs were normal, and physical exam was unremarkable. Troponin trend was negative and EKG with normal sinus rhythm. Calcium was elevated to 11.1 mg/dL. Computed tomography (CT) angiography of the chest showed a moderate to large anterior mediastinal hematoma with suspected left sided mass with blush, consistent with active extravasation (Image 1). It also showed hemorrhagic bilateral pleural effusions and a small pericardial effusion. The aorta and thoracic arterial vasculature were unremarkable. She denied anticoagulation and NSAID use. The patient was initially hemodynamically stable, so cardiothoracic surgery opted for conservative management in the ICU with chest tube placement for the left hemothorax. Magnetic resonance imaging of the chest with contrast confirmed an anterior mediastinal mass 3.2cm in size. There was no evidence of metastatic disease on CT abdomen and pelvis. Tumor markers lactate dehydrogenase, alpha-fetoprotein, beta-human chorionic gonadotropin were within normal limits.Subsequently, her hemoglobin dropped from 13 g/dL to 7.3 g/dL with symptomatic fatigue and tachycardia. Patient underwent a median sternotomy with resection of the mediastinal mass. Operative findings included an extensive hematoma ventral to the main pulmonary trunk that dissected through mediastinal fat and thymic tissue. Pathology revealed a 4 cm intrathymic parathyroid adenoma, associated with a large organizing hematoma and fibrosis (22 x 11 x 4 cm, Image 2).Patient recovered without complications.
Discussion: Parathyroid adenomas are the most common cause of primary hyperparathyroidism, noted primarily in patients with refractory and recurrent hyperparathyroidism. If symptomatic, parathyroid adenomas are generally resected. If asymptomatic, they are occasionally resected, otherwise, are monitored with annual screening of serum calcium, creatinine, and bone density. Parathyroid adenomas are highly vascularized, with fragile blood vessels and, have an increased risk of spontaneous mediastinal hemorrhage. Surgical intervention is typically required in these patients.The location of parathyroid adenomas is primarily in the neck, however, in 8.5-16% of cases, parathyroid adenomas are found ectopically1-2. Ectopic parathyroid glands form during embryonic development due to an aberrant migration of the third and fourth brachial pouches. Given that both the thymus and the parathyroid glands are derived from endoderm, it is possible for parathyroid glands to be found within the thymus gland.
Conclusions: Here, we discuss a 32-year-old female who presented with chest pain and recent ecchymoses. She was found to have an atypical presentation of an ectopic parathyroid adenoma which was complicated by a large organizing hematoma and fibrosis, bilateral hemorrhagic pleural effusions, and a pericardial effusion. Perioperatively, she presented with no symptoms of hypercalcemia or hypophosphatemia. Careful management and localization of ectopic parathyroid adenomas is important and can pose a unique surgical challenge, especially in patients with hemorrhagic complications.