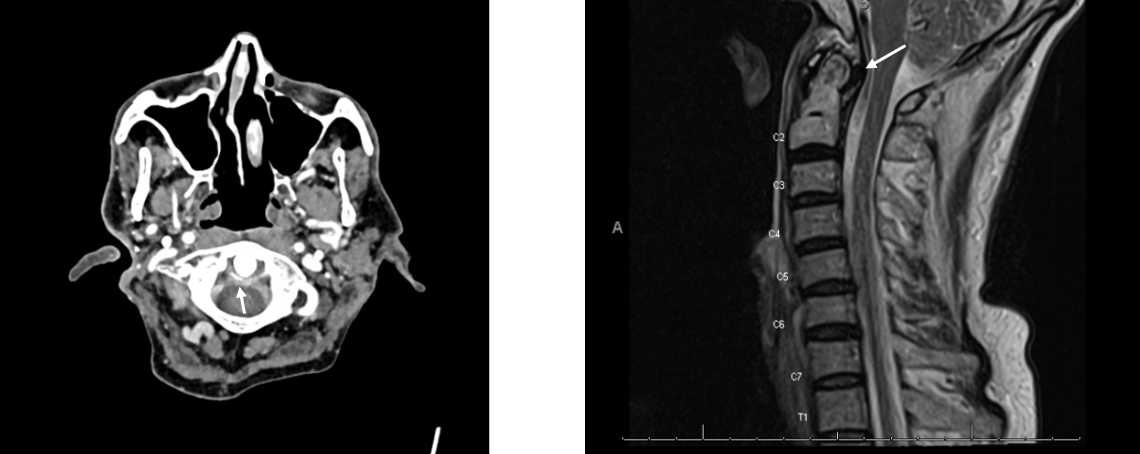
Case Presentation: A 58-year-old man with HIV on treatment, hepatitis C infection, prior liver transplant (2006) on cyclosporine, atrial fibrillation, CKD stage III, and gout was admitted to the hospital with 48 hours of nuchal rigidity, headache, and fevers up to 101.4 F. He disclosed recent dry needling of his neck and upper back. Exam was notable for nuchal rigidity, decreased range of motion in the cervical spine, and swelling, warmth, and erythema of the right elbow with diminished range of motion. Labs were notable for WBC 9.4, Cr 1.78 (baseline 1.3), normal lactate, and CD4 count 460. LP was performed and was normal with WBC< 3. On hospital day 2, arthrocentesis of the right elbow revealed WBC 78,000 with 92% PMN and intracellular crystals characteristic of calcium pyrophosphate (CPP), confirming the diagnosis of pseudogout, or calcium pyrophosphate deposition disease (CPPD). Blood and CSF cultures were negative. Cervical spine CT showed calcium around the dens suggesting calcification of cartilage and ligaments (Figure 1a). MRI showed pannus formation at C1/2 (Figure 1b). Rheumatology was consulted, and the patient was diagnosed with polyarticular CPPD flare involving the cervical spine and elbow. He was treated with prednisone 40 mg daily starting on hospital day 3, experienced marked improvement in cervical pain and range of motion within one day and was continued on a steroid taper with resolution of symptoms.
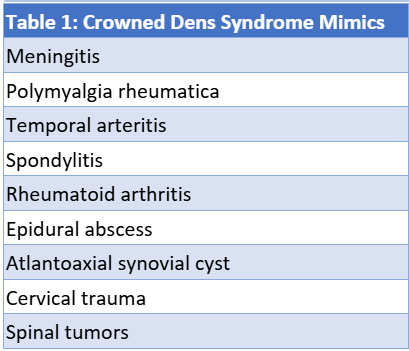
Discussion: The constellation of neck pain, nuchal rigidity and fever in an immunocompromised patient was concerning for meningitis. However, in the context of a reassuring LP, the clinical presentation, synovial studies, imaging findings, and rapid response to steroids ultimately supported the diagnosis of an uncommon subtype of CPPD, known as crowned dens syndrome (CDS). Typical features of CDS, where CPP deposition occurs on the dens of C2, include neck pain, fever, elevated ESR/CRP, characteristic imaging findings (Figure 1a) and is typically very responsive to treatment with NSAIDs or steroids [3]. CDS is thought to be rare, though its precise incidence is unknown. It is estimated that CPPD affects 10% of people aged 60 years and older [1]. The frequency of dens calcification in those with CPPD is about 50%, and only about 25% of people with CPPD experience a pseudogout flare [2]. The clinical presentation has many mimics (Table 1), and it is estimated that up to 50% of cases of CDS are initially misdiagnosed with an average diagnostic latency of 7 days [3]. In this case, early consideration with imaging and Rheumatology consultation allowed prompt diagnosis and rapid improvement.
Conclusions: Crowned dens syndrome is a rare and underrecognized mimic of meningitis, characterized by acute neck pain, nuchal rigidity, and fever due to calcium pyrophosphate deposition around the odontoid process. It is an important differential diagnosis that is infrequently considered despite risk factors such as immunocompromise, age, or a history of gout or pseudogout. Early consideration of spinal imaging to support the diagnosis and prompt initiation of treatment can avoid the need for more invasive diagnostic testing and shorten hospitalization.