Background: Chronic obstructive pulmonary disease (COPD) is a progressive respiratory disorder characterized by persistent symptoms and partially irreversible airflow limitation, leading to reduced exercise capacity, respiratory failure, and death 1. COPD affects over 16 million Americans and is a major cause of morbidity and mortality worldwide. In the US, it is the 5th leading cause of death. Acute exacerbations often lead to hospitalization, with over 750,000 annual admissions 2.In 2011, the 30-day readmission rate for patients with COPD was 22%; it was associated with lower quality of life, reduced functional capacity, increased mortality, and higher health care costs. Up to one-third of these readmissions are considered preventable 3. Recent data from New York report a similar 30 day all cause readmission rate of 22% among patients with COPD 4.Integrated care models, such as discharge coordination, supported self-management, early discharge programs, telemedicine, and discharge education have been developed to reduce readmissions. Discharge rehabilitation, supported self-management, and coordinated discharge interventions appear most effective 3.We report on our institution’s first year of experience participating in The Virtual Mentored Implementation to Reduce REVISITS (Reducing Respiratory Emergent Visits using Implementation Science Interventions Tailored to Setting) Study, a nationwide, multi-center trial evaluating interventions to reduce unplanned emergency visits for COPD 5.
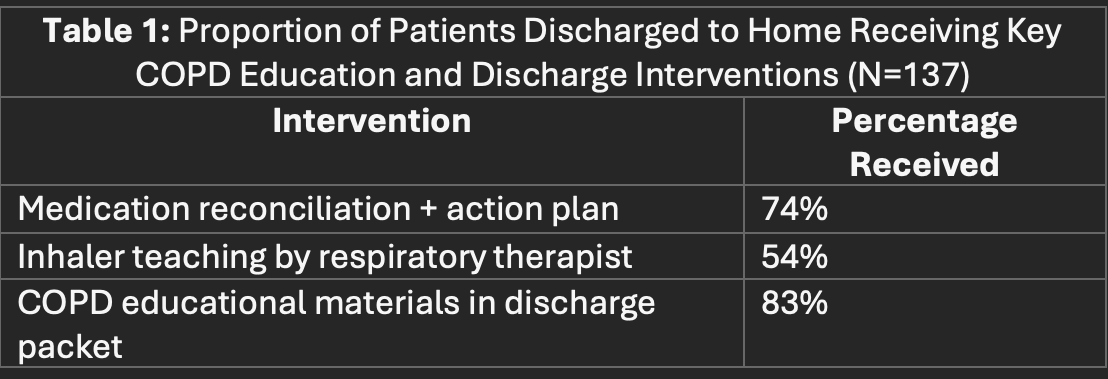
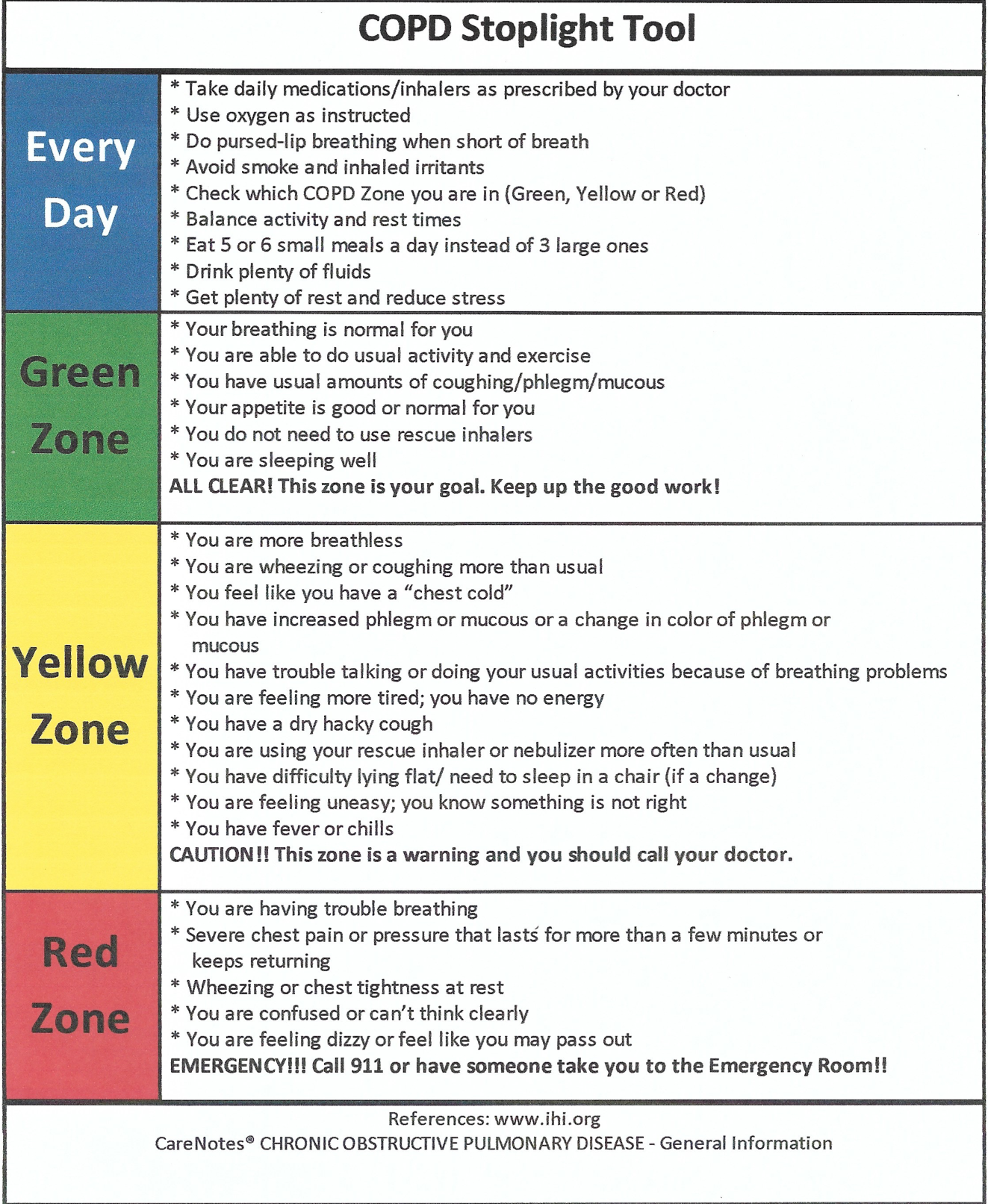
Methods: Adults with acute COPD exacerbations (AECOPD) were identified using hospital admission diagnosis codes. We developed a three-part intervention bundle for patients hospitalized with AECOPD: inhaler education during hospitalization, and medication reconciliation and review of a COPD action plan 6 after discharge.Respiratory therapists provided individualized education on inhaler use, including device identification, step-by-step instruction, and supervised self-administration. After discharge, we contacted patients by phone to review medications and the COPD action plan. All interventions and outcomes were recorded in a deidentified data system. We report on our reach for delivering our quality improvement bundle, as well as our observation of COPD readmission rates at our hospital before and after our intervention period.
Results: From June 2023 to March 2024, there were 167 AECOPD admissions among 137 patients. Most patients were discharged home (84%); others went to skilled nursing facility (11%), hospice (4%), or were transferred (1%). Of 141 home discharges, 74% were contacted, 5% were readmitted before being contacted, and 20% were unreachable after two phone calls. Only 2 patients (1%) declined to participate in the post-discharge phone interview. The mean and median time to contact was 8 days, with a range of 1-18 days. 30% of the encounters received all interventions, and only 5% did not receive any intervention. Only 1 readmitted patient received the full bundle. The COPD-specific 30-day readmission rate reported by our institution was 14.29% for the year prior to implementation. During the implementation year, our hospital reported a COPD-specific 30-day readmission rate of 11.86%.
Conclusions: A bundle of interventions including inhaler education, medication reconciliation, and action plan review was delivered to patients with AECOPD and correlated with a decreased 30-day COPD-specific readmission rate during the first year of implementation.