Background: Hospitals nationwide are implementing throughput initiatives to optimize bed capacity and reduce avoidable length of stay. A common strategy involves asking interdisciplinary team members to identify and escalate barriers to discharge in real time. Although prior studies describe common types of discharge barriers, little is known about how different inpatient team members conceptualize and prioritize these delays. To inform more effective multidisciplinary throughput strategies, we sought to characterize how members of the inpatient care team perceive and prioritize common barriers to discharge.
Methods: We conducted an anonymous online survey of inpatient interdisciplinary team members at a university-affiliated health system in September 2025. The survey assessed perspectives of clinical or logistical barriers to advancing care that caused a delay in discharge, defined as any barrier that causes a patient to leave later in the day than expected or that adds one or more extra days to their hospital length of stay. It was distributed via institutional email listservs and unit-based leadership, and participation was voluntary. Respondents indicated their primary role and clinical service and then ranked discharge barriers from a predefined list according to (1) which they encountered most frequently and (2) which they perceived as most important to address proactively to avoid discharge delay. Top five barrier rankings were compared qualitatively across interdisciplinary groups to identify areas of overlap.
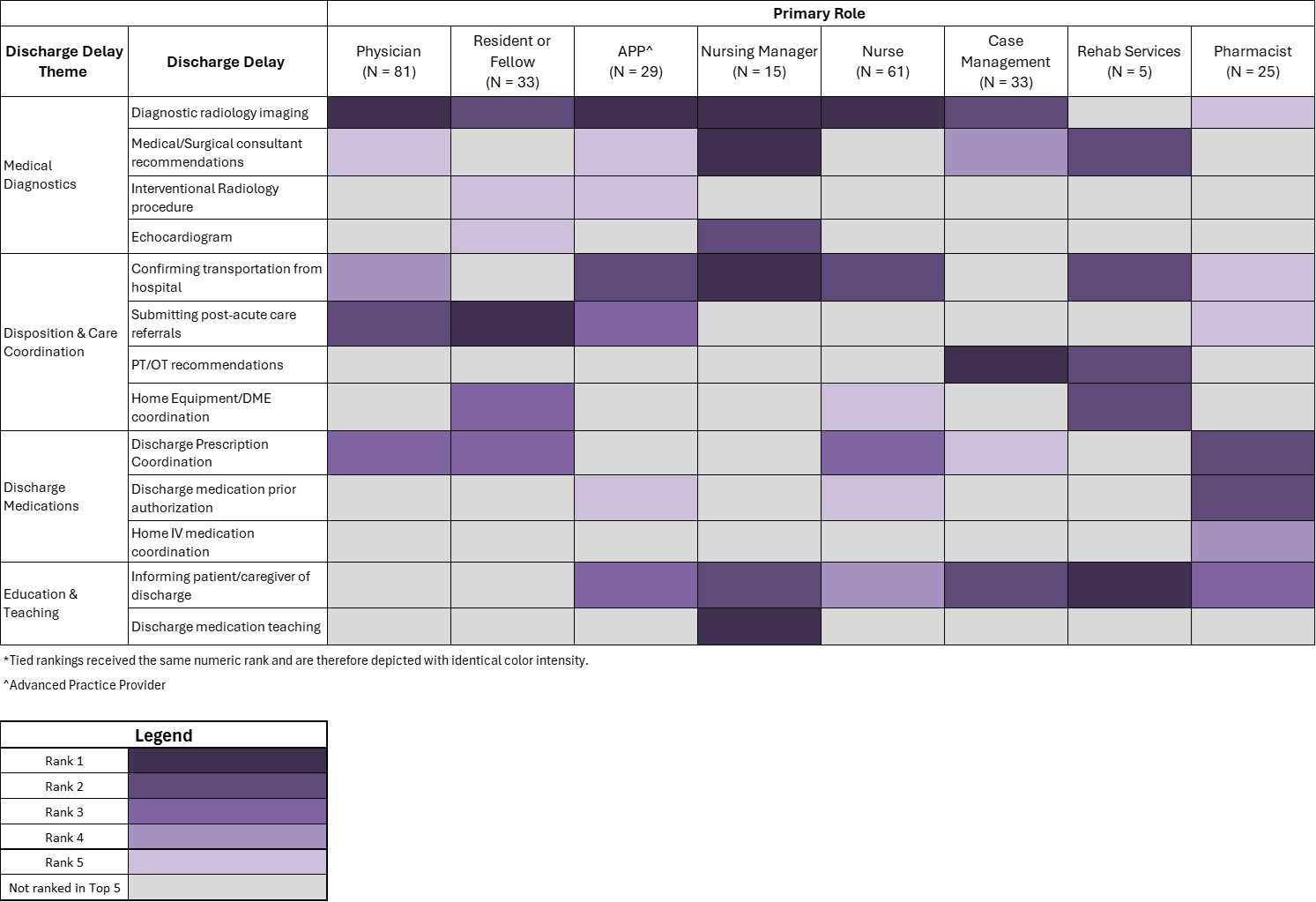
Results: Two hundred eighty-two individuals participated in the survey. The highest participation came from attending physicians (29%), followed by nurses (22%), residents and fellows (12%), and case management (12%). The remaining 25% of responses were from advanced practice providers, pharmacists, nursing managers, and rehab services. Among physicians (including residents and fellows), Hospital Medicine was the highest represented service (57%). While the top five rankings of most frequently encountered discharge barriers varied somewhat across groups (Table 1), several barriers – diagnostic imaging, hospital transport confirmation, prescription coordination, and consultant recommendations – were consistently identified across disciplines. Rankings of most important barriers to address proactively largely mirrored frequency ratings (Table 2), with submitting post-acute care referrals and informing patients/caregivers of expected discharge more prominently prioritized. Diagnostic imaging was the most common top-ranked delay in both frequency and importance to address proactively across roles.
Conclusions: Despite some variation in how interdisciplinary team members rank and prioritize discharge delays, several barriers emerge as shared pain points across roles. Individuals generally ranked barriers similarly in both frequency and importance to address proactively, indicating broad agreement that the most frequently encountered barriers are also viewed are the most pressing to address. These areas of alignment represent high-yield targets for designing systemwide tools and workflows to support timely identification and escalation of discharge barriers, and may serve as a foundation for more aligned throughput improvement efforts.
.png)