Background: Left Atrial Enlargement (LAE) is a known predictor of cardiovascular morbidity and mortality. Prior to cardiac point-of-care ultrasound (POCUS), LAE was assessed mainly by cardiologists via echocardiogram. Previous studies evaluating visual estimation of left atrial (LA) size in the parasternal long axis (PLAX) view showed modest test characteristics but used older echocardiographic reference ranges. The objective of this study was to evaluate novel techniques for detecting moderate to severe LAE in the apical 4 chamber (A4) and apical 2 chamber (A2) views using newer reference ranges and done by POCUS providers in Hospital Medicine.
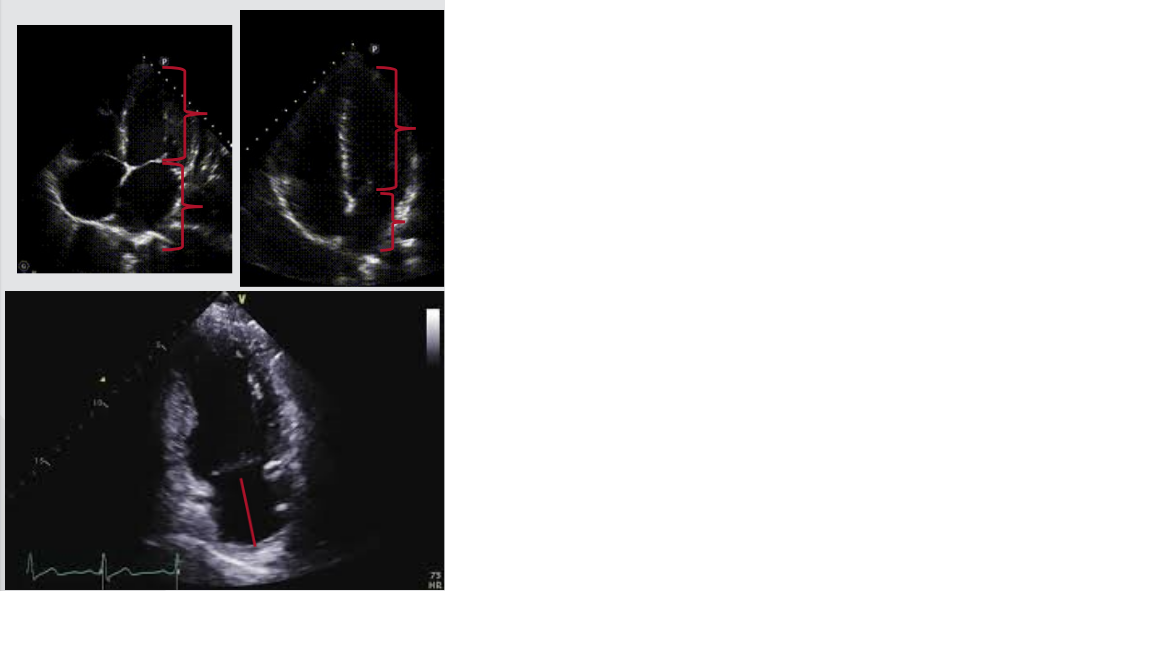
Methods: Consecutive adult transthoracic echocardiograms (TTE) performed at Nebraska Medicine were reviewed for the study. Exclusion criteria included duplicate exams from the same patient, missing LAVI data, and altered cardiac anatomy. A power analysis determined sample size. TTE images were de-identified and exported for review by 3 blinded hospital medicine faculty with POCUS expertise. Images in the A4 and A2 views were evaluated using 3 strategies. Images were first evaluated via an “eyeball” method by comparing the LA to the left ventricle (LV). If at any point in the cardiac cycle the LA was < 1/3 of the total length of the heart, LA size was considered normal (i.e. no LAE). Next, the LA length was measured in end-ventricular systole. Two different cut-points (5 cm and 6 cm) were evaluated for identifying LAE. Data were analyzed using SAS v 9.4. Descriptive statistics were used to summarize the patient characteristics. Test characteristics, including sensitivity, specificity, predictive values, and likelihood ratios, were calculated for each LAE assessment technique.
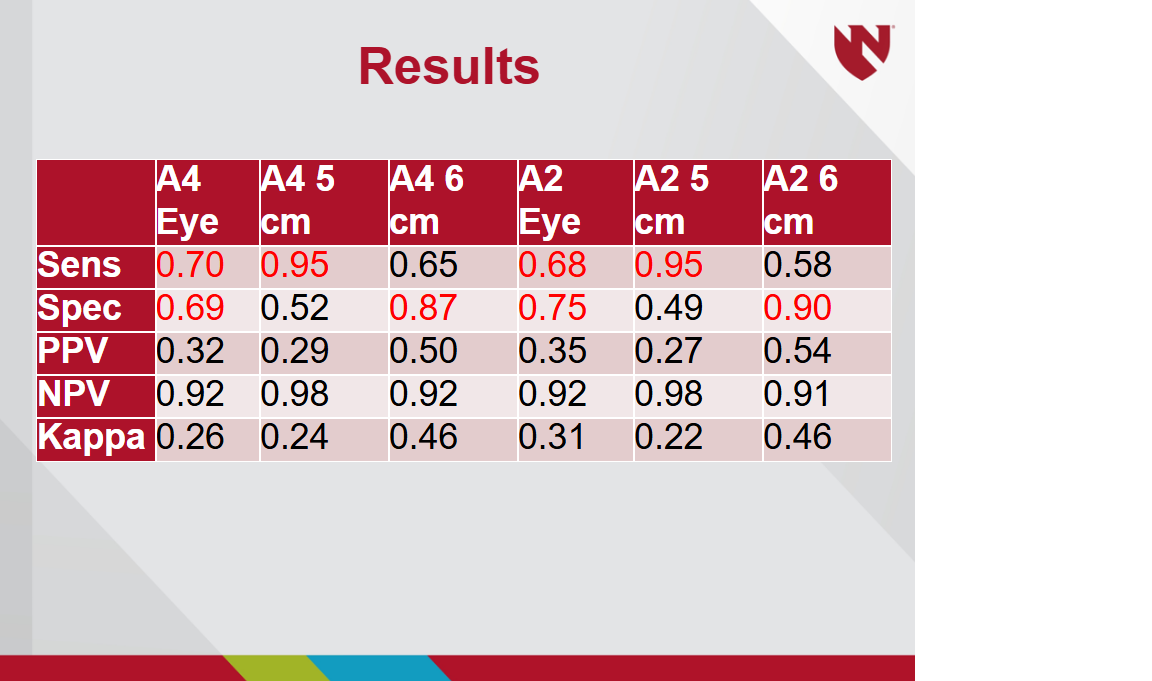
Results: A total of 321 TTE exams were reviewed with 80 (25%) meeting exclusion criteria, resulting in 241 exams included in the analysis. Approximately 15% had moderate to severe LAE by LAVI measurement. In the A4 view, visual estimation of LA:LV length had sensitivity of 70%, specificity of 69%, PPV 32%, NPV 92%, LR+ 2.3, LR- 0.4. LA length >5 cm had sensitivity of 95%, specificity 52%, PPV 29%, NPV 98%, LR+ 2, LR- 0.1. LA length >6 cm had sensitivity 65%, specificity 87%, PPV 50%, NPV 92%, LR+ 4.9, LR- 0.4. Index test characteristics were similar in the A2 view. The inter-rater reliability values for index tests were approximately kappa=0.5.
Conclusions: Screening for LAE with POCUS using the eyeball method in A4 and A2 proved to have similar test characteristics as previously reported PLAX eyeball methods and used newer echocardiographic left atrial volumetric indices for measuring LAE. This novel technique could be used to assess LAE as an adjunct to PLAX or if the PLAX view is unobtainable. Using caliper measurements in A4 and A2 showed differing test characteristics than the eyeball method. Using a cutoff of < 5 cm showed test characteristics that would be helpful in ruling out LAE. Using >6 cm showed test characteristics helpful in ruling in LAE.