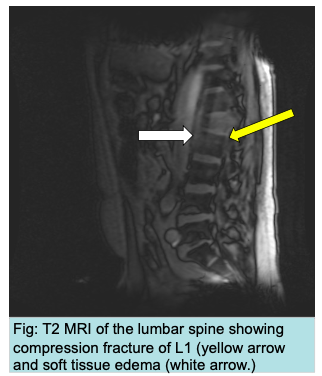
Case Presentation: A 57-year-old African American man with a past medical history of alcohol use disorder, treatment naive chronic hepatitis C infection, and epilepsy presented with left flank pain without urinary symptoms. A non-contrast abdominal CT scan did not show renal pathology but showed compression fracture the L1 vertebra with paravertebral soft tissue and stranding. He was treated with calcitonin, opiates, and kyphoplasty for presumed alcohol-related osteoporosis. In addition to the L1 acute compression fracture, an MRI showed mildly enhancing paraspinal soft tissue and an area of enhancing marrow abnormality in L2 (Figure 1). Biopsy of the soft tissue showed the presence of adenocarcinoma of prostatic origin.
Discussion: This unfortunate and unique case underscores multiple learning points. Although prostate cancer is well known for metastatic osteosclerotic bony lesions, osteolytic lesions can also occur, hence the diagnosis should be entertained in patients with osteolytic lesions of unknown source. The case also highlights the importance of collecting and publishing data on patients presenting with advanced regional or metastatic prostate cancer following the USPSTF recommendation against screening. High risk populations mostly individuals of African American descent and those with family history of the disease are high priority for detailed counseling. Finally, patients with vertebral compression fracture can present with flank pain with minimal midline pain. The diagnosis should be considered in those with no urinary symptoms and negative urinalysis.
Conclusions: PSA screening for prostate cancer may reduce risk of prostate cancer mortality but is associated with harms including false-positive results,biopsy complications and over diagnosis in 20-50%. Following the 2012 USPSTF recommendations against screening for prostate cancer, there has been a notable decline in the diagnosis of new cases of prostate cancer. However, this comes at the expense of more patients presenting with advanced metastatic disease. Further studies are needed to determine better protocols for optimizing rather than eliminating screening, such as utilizing MRI imaging, free PSA levels, or PSA velocity. It would be beneficial for future research to focus on certain markers to distinguish between more indolent or more aggressive prostate cancers and thus eliminating over treatment harms.