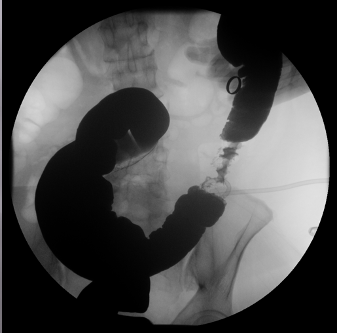
Case Presentation: A previously healthy 54-year-old African American woman with a history of chronic constipation and tobacco use disorder presented to the emergency department with a 3-day history of intermittent left lower quadrant (LLQ) cramping abdominal pain which radiated to her back and an associated 5-day history of fatigue. She had no prior colonoscopy. On presentation, patient was afebrile and hemodynamically stable. Her physical exam was notable for mild LLQ tenderness on deep palpation without rebound or guarding. Initial lab work was significant for a mild leukocytosis (WBC 10.8 with neutrophilic predominance) and a microcytic anemia (Hgb 7.4, MCV 76.4). Iron panel was suggestive of anemia of chronic disease (serum iron 16, total iron binding capacity 190, iron saturation 8%, ferritin 326). Her stool occult blood was negative. A non-contrast CT abdomen and pelvis showed acute colitis in her descending and sigmoid colon and a left psoas abscess. Her psoas abscess was drained surgically and grew gram positive rods, gram negative rods and anaerobes. A mixed culture suggested gastrointestinal or genitourinary etiology, hence, a flexible sigmoidoscopy was performed which showed a malignant appearing stricture in the sigmoid colon which was biopsied. Barium enema revealed a 6 cm segment of persistent narrowing at the junction of sigmoid and descending colon with associated mucosal irregularity and shouldering (apple-core lesion). Pathology report revealed an invasive moderately differentiated adenocarcinoma of the colon. Patient underwent left colectomy followed by adjuvant chemotherapy. Patient was then discharged home in a stable condition with recommendations to repeat colonoscopy in 3 months for surveillance.
Discussion: Psoas abscess is a rare infectious disease and can present with vague clinical features, such as fever and back pain. It is classified as primary or secondary and is associated with various clinical conditions such as Crohn’s disease, diverticulitis, appendicitis, vertebral osteomyelitis, urinary tract infection and endocarditis. Its insidious onset and occult nature frequently causes diagnostic difficulty. Hence it is important to keep in mind that there could be an underlying serious pathology presenting as psoas abscess.
Conclusions: This case illustrates the significance of recognizing atypical presentations of serious underlying diseases such as development of a secondary psoas abscess in the setting of an underlying colon cancer perforating into a psoas muscle. Hence, besides treating psoas abscess with antibiotics and incision and drainage, efforts should be made to identify the primary cause to catch the underlying disease as early as possible. A delay in diagnosis of conditions like cancer can lead to worse outcomes with increased rates of morbidity and mortality.