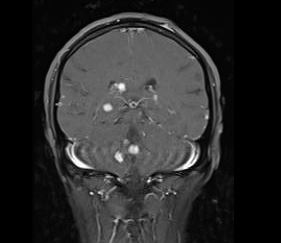
Case Presentation: A 29-year-old African American male with no prior past medical history initially presented to the Orthopedics clinic for evaluation of multiple soft tissues masses. They had been present over all four extremities as well as the back and had been progressively increasing in number. Due to pruritis patient would scratch them and they would bleed and then scab over. Also had bony pain in numerous locations including his left hand, right knee and bilateral wrists. He complained of a 6 month history of blurry vision and also endorsed 15 pounds of unintentional weight loss over last few months. No reported fevers, trauma, foreign travel. A left forearm mass was biopsied and revealed non caseating granulomatous inflammation with no neoplastic changes but did reveal yeast on the smear. Patient was referred to hospital for concerns for systemic fungal process. On examination patient had multiple 2-3 cm soft tissues masses over all the extremities with some having ulcerations or scabs. There was bilateral small cervical lymph nodes palpated along with axillary and inguinal lymphadenopathy. Ophthalmological exam revealed exposure keratitis and iritis. Initial labs showed only mild normocytic anemia. X-rays of bilateral forearms were obtained and revealed multiple bony lytic lesions in both upper extremities. Neuroimaging showed multifocal bihemispheric cervical cord, intra-orbital and intrasinus lesions along with infiltrative masses in bilateral lacrimal glands. CT chest showed mediastinal, perihilar, and bilateral axillary adenopathy. ACE levels were checked and were elevated. Given the constellation of clinical symptomatology and results of imaging studies along with pathology the diagnosis of disseminated sarcoidosis was established. Therapy was initiated with intravenous steroids and discharged on high dose oral steroids and topical ocular steroids with outpatient close follow up.
Discussion: Disseminated sarcoidosis is an uncommon entity that is encountered in the hospital setting. Hospitalists should be cognizant of this diagnosis as this is a differential of systemic disease processes particularly fungal infections. Hence infectious processes need to be ruled out before therapy with high dose steroids can be initiated. Without treatment the disease can progress can lead to devastating complications. Diagnosis involves clinical signs and imaging supportive of sarcoidosis plus histopathology revealing non caseating granulomas along with exclusion of other diseases that produce granulomas. Treatment involves systemic steroids and close follow up to monitor for complications and further progression.
Conclusions: Sarcoidosis is a multisystem pathological process that can impact any organ in the body with varying presentations. Hence this should be recognized as a potential differential for systemic disease processes.