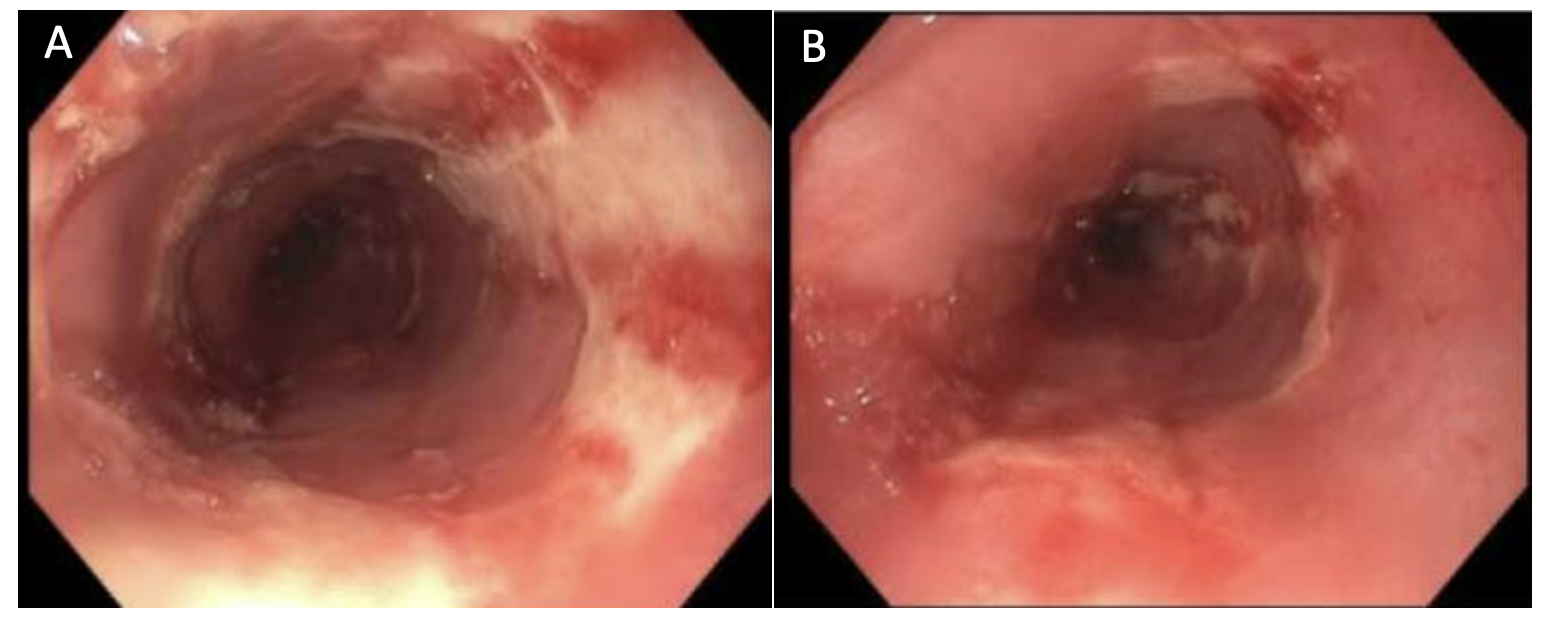
Case Presentation: A 22-year-old woman with history of recurrent sinusitis was admitted with hypoxia, shortness of breath, severe subacute odynophagia, and dysphagia. She was given cefuroxime by her otolaryngologist for a suspected sinus infection earlier in the month, with no effect. She then developed white plaques over her lips and tongue and a severe cough. She was diagnosed with bronchitis and oral thrush and given both fluconazole and prednisone. The following day, she developed blisters over her lips, lesions within her mouth and vagina, and blurry vision. She went to the urgent care, where she received amoxicillin and an ophthalmic ointment. Her symptoms persisted despite the antibiotics, and she also developed severe shortness of breath, prompting her arrival to our emergency department, where she was evaluated and discharged on standard antibiotics for suspected community-acquired pneumonia. She returned two days later after no improvement and was admitted. The primary team rapidly initiated an interdisciplinary approach. Dermatology was consulted for her mucosal lesions. Gastroenterology was consulted for her severe odynophagia and dysphagia. An esophagogastroduodenoscopy (EGD) revealed several superficial semi-circumferential and fully circumferential esophageal ulcers (Panel 1) that were not biopsied due to perforation risk. Dermatology suggested considering reactive infectious mucocutaneous eruption (RIME) based on timeline of medication use and morphology of lesions. Her initial chest x-ray was negative for consolidations, but a respiratory viral polymerase chain reaction resulted positive for Mycoplasma pneumoniae. She was initiated on intravenous steroids, eventually transitioned to oral steroids, and discharged on a minced and moist diet.
Discussion: RIME is commonly associated with Mycoplasma pneumonia infection and characterized by prominent mucositis with or without cutaneous involvement. It is a rare cause of subacute dysphagia and odynophagia among young adults [1]. RIME commonly affects younger populations, with a mean age of 16 years old [2], and some experts suggest making young age a diagnostic criterion due to the rarity of this condition in adults. The exact pathogenesis of RIME remains unknown. It is thought that Mycoplasma infection is associated with increased systemic inflammation and prolonged surface colonization due to nonspecific interactions between the mycoplasma bacterium and host cells [3]. In this patient’s case, it was likely that the interactions between the mycoplasma bacterium and the esophageal mucosal layers led to extensive immune complex deposition and ulcer formation, causing significant odynophagia.
Conclusions: Although of different etiologies, RIME, Stevens-Johnson syndrome (SJS), and erythema multiforme (EM) have similar manifestations. They can all present with cutaneous and mucosal lesions. For all three conditions, inpatient supportive care remains the mainstay of management. Intravenous steroids can be utilized for severe RIME, as seen in our patient. Alternative means of nutrition are frequently required due to the degree of odynophagia that severe RIME can cause. The degree of esophageal involvement seems to correlate to the severity of RIME. This unique case further highlights the importance of early interdisciplinary care with the primary team involving both Dermatology and Gastroenterology to expedite the initial evaluation of this patient’s symptoms, which lead to a more rapid diagnosis and appropriate therapy.