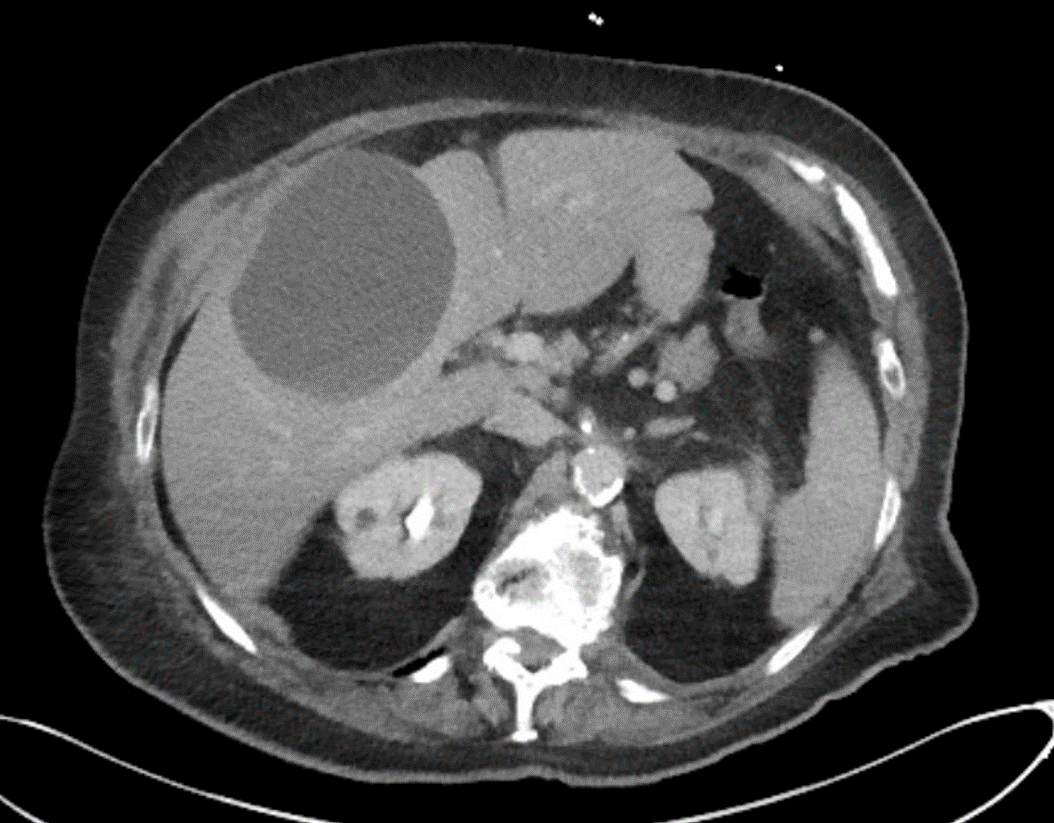
Case Presentation: A 92 year old female with a PMH significant for occipital neuralgia, glaucoma, cataracts, HTN, HLD, chronic lower extremity edema, and GERD presented to the ED with complaints of headache, cough, congestion, and RUQ pain. She had no history of tobacco or drug use. Her medications included Gabapentin, Tylenol, Tramadol, Losartan, Simvastatin, Lasix, and Pantoprazole. She had allergies to Penicillin, Levaquin, and Cephalosporins. On arrival to the ED she had a low grade fever of 99.4F in the setting of recent Tylenol intake. She was also found to be hypoxic with O2 sat 90% on room air. On initial exam, her lungs were clear to auscultation but otherwise notable for systolic murmur and RUQ tenderness without rebound or guarding. Imaging was unremarkable other than right hepatic lobe simple cyst measuring up to 9.9 cm. Labs were unremarkable other than COVID-19 PCR positive and urinalysis with pyuria. She was admitted for management of COVID and presumed UTI. She was treated with Remdesivir and steroids as well as supportive care with supplemental oxygen for treatment of COVID. She was treated with Bactrim for presumed UTI which was discontinued once her urine culture resulted with 10-50k mixed organisms resembling urogenital flora. After completing treatment for COVID she developed increasingly higher fevers and blood cultures were found to be positive for E.Coli. She was also found to have new LFT elevations. A repeat CXR demonstrated mild to moderate pulmonary edema with cardiomegaly associated with small lateral pleural effusions and increased patchy opacities in both lower lobes indicating atelectasis versus pneumonia. A RUQ ultrasound demonstrated mild fatty infiltration of the liver with a large complex right lobe cyst. She was started on IV Ertapenem for treatment of her bacteremia with presumed source thought to possibly be secondary to pneumonia as no urinary, skin, or other source was identified. A TTE was sent to further evaluate her systolic murmur which demonstrated vegetation on her aortic valve. The patient did not improve clinically with persistent waxing and waning fatigue and lethargy as well as persistent leukocytosis. As such, a repeat CT A/P was sent demonstrating an enlarging right hepatic lobe collection with new rim enhancement representing abscess. She underwent IR drainage with placement of a hepatic drain and was continued on IV Ertapenem.
Discussion: The patient presented with RUQ pain which persisted and was attributed to a variety of etiologies, many of which stemmed from assumptions surrounding potential diagnoses being considered such as costal pain from coughing or referred pain from pyelonephritis. This symptom wasn’t explored further likely due to availability bias and search satisfying. Availability bias occurs when individuals rely on recent or easily-recalled examples when making a decision. Availability bias played a role in this case as providers frequently treat diagnoses of COVID and UTI, though it is rare to treat a patient with a hepatic abscess which has an incidence of 0.0023%. Search satisfying is the tendency to stop searching once a plausible explanation is found. Search satisfying played a role in this case as alternative diagnoses were not considered once data from initial ED workup returned with positive COVID-19 PCR and pyuria on urinalysis.
Conclusions: Understanding the role cognitive biases play in clinical decision making can help providers reduce the risk of making diagnostic errors and improve patient quality and safety.