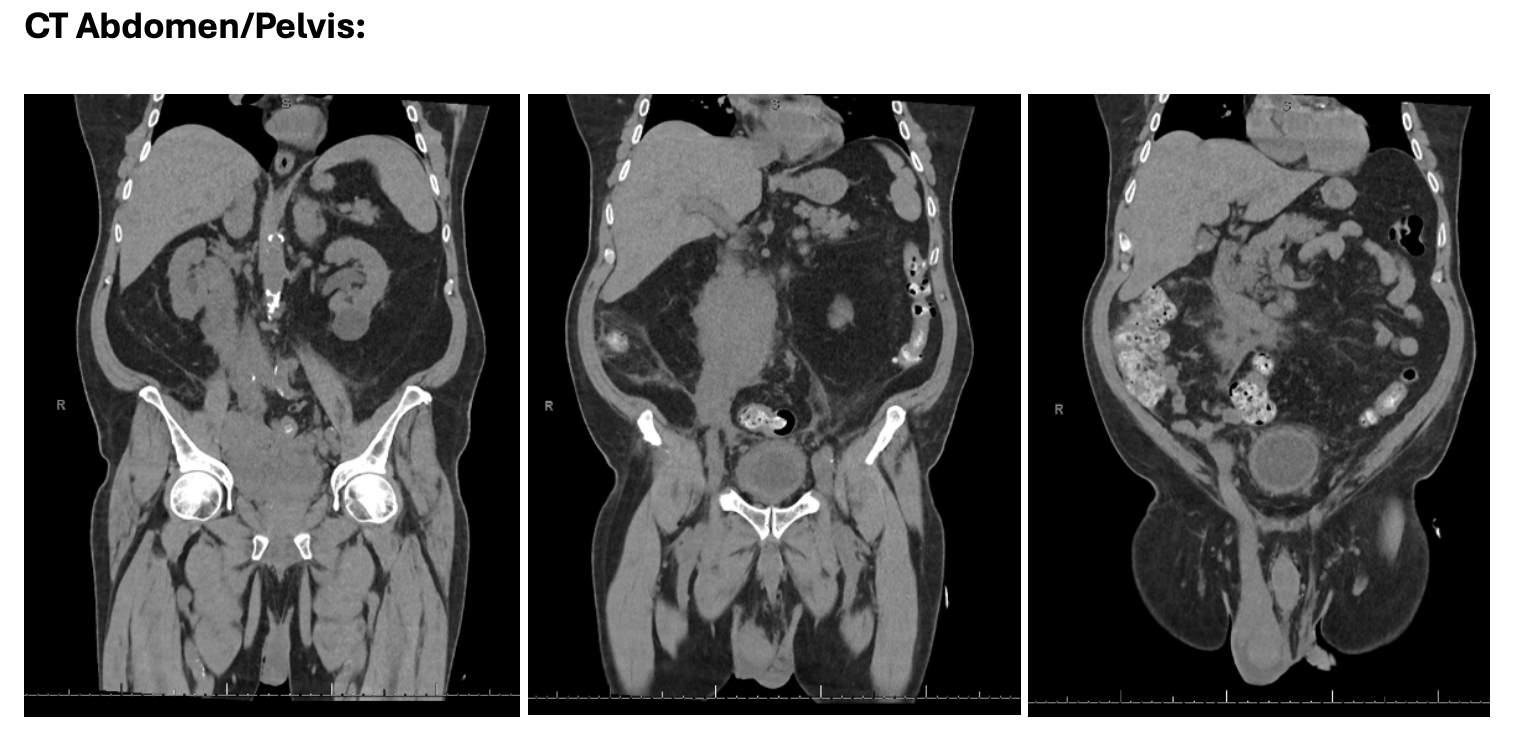
Case Presentation: A 79 year old male presented to the hospital for evaluation of acute worsening testicular pain/swelling that had been ongoing for 3 months. When symptoms first began three months prior, he was evaluated by Urology and diagnosed with epididymitis; however, he completed two courses of antibiotics without symptomatic improvement. Testicular and abdominal ultrasound exams in the outpatient setting at that time were largely unremarkable. A few days prior to presenting to the hospital, his primary care provider ordered a CT abdomen/pelvis to evaluate the ongoing pain which showed evidence of widely metastatic cancer of unknown primary involving the genitourinar system, adrenals, lymph nodes, liver, omentum, and expansion within the IVC/gonadal vein. These results prompted his current hospital presentation. A repeat testicular ultrasound in the emergency department showed findings consistent with epididymitis and orchitis. Initial labs were unrevealing, and vital signs were within normal range. He was admitted for further evaluation and management. Further lab evaluation revealed undetectable human chorionic gonadotropin, low testosterone (24), appropriately elevated luteinizing hormone (15.8), iron deficiency, elevated lactate dehydrogenase (1,112), and normal random serum protein electrophoresis, prostate specific antigen, alpha fetoprotein, follicle-stimulating hormone, folate, uric acid, phosphorous, and haptoglobin. MRI brain was normal. PET/CT showed FDG avidity at the right testis concerning for primary site of malignancy with extensive metastatic disease. CT guided biopsy of retroperitoneal lymphadenopathy revealed diffuse large B-cell lymphoma (DLBCL), non-germinal cell type, EBV negative, and Ki-67 proliferation index of 90%. The malignant hematology service was consulted, a port-a-cath was placed, and patient was initiated patient on R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) and intrathecal (IT) methotrexate (MTX). Lumbar puncture did not reveal evidence of clonal lymphoproliferative process. He was discharged 5 days after receiving initial chemotherapy and with close oncology follow up.
Discussion: Primary testicular lymphoma (PTL) is a rare, clinically aggressive form of extra nodal lymphoma accounting for less than 5% of testicular malignancies and only 1-2% of non-Hodgkin lymphoma (NHL) cases (1). PTL is most commonly seen in males in the 6th decade of life. Testicular involvement of DLBCL is associated with adverse prognosis and increased risk for central nervous system (CNS) involvement, which alters the typical DLBCL treatment regimen due to the need to include IT MTX in addition to R-CHOP for CNS prophylaxis (2).
Conclusions: This case highlights the importance of considering PTL in men greater than 60 years of age who present with scrotal pain, particularly if symptoms fail to improve on initial therapies, such as antibiotics, in order to avoid a delayed or missed diagnosis and delayed treatment.