Background:
Multiple tools have been developed to improve the quality of signout from daytime clinicians to night covering clinicians. However, despite the frequency of holdover signout (new overnight admissions whose care is transferred to a new primary team), there are no studies or generally accepted best practices to ensure a high quality new admission handoff.
Purpose:
To improve the safety, efficiency, and educational quality of holdover signout by testing and implementing a structured holdover framework.
Description:
In Sept-Nov 2014, we conducted a needs assessment consisting of 61 directly observed holdover signouts, 6 structured interviews and 5 focus groups with hospitalists and residents. We identified that:
- Signout consisted mostly of H&P presentations that repeated information available in the electronic medical record (EMR)
- Day teams receiving signout had limited opportunity to engage in the specifics of diagnostic uncertainty or plan of care
- Night residents received little to no education or feedback on their clinical decision making
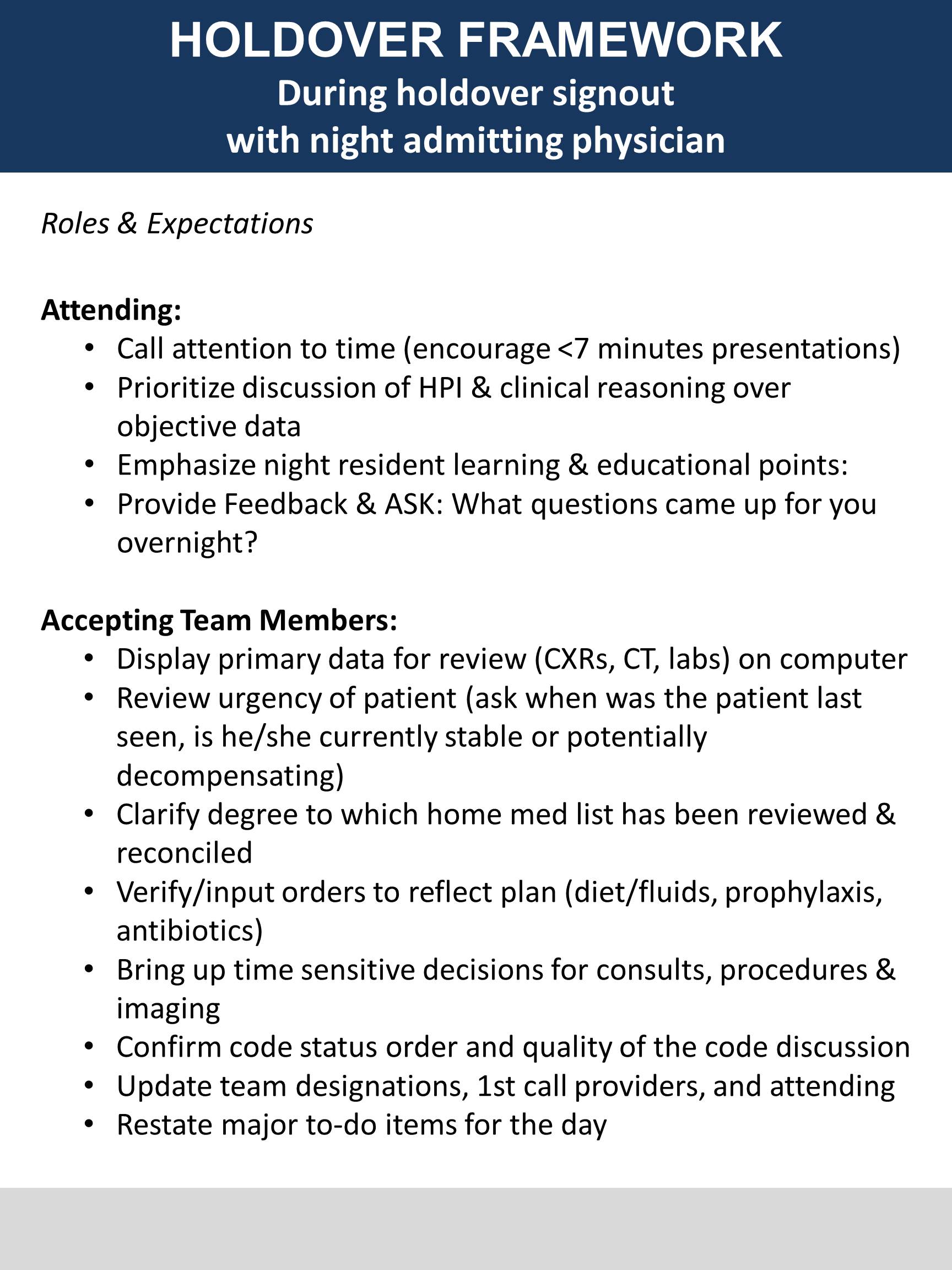
From our findings, we developed a standardized framework for holdover signout (Figure 1), which requires computer use to access our EMR during handoffs. In March 2015, we targeted 4 teams on the internal medicine teaching service to pilot the framework. We observed the same parameters as in our initial needs assessment. Time spent repeating data found in the EMR decreased from 57% to 22% of total signout time, and frequency of teaching moments and feedback on overnight medical management increased from 33% to 93%. We also received positive qualitative feedback from residents and attendings.
In August 2015, we expanded the pilot to all teaching teams, promoting the framework through our weekly faculty meeting, large posters in signout rooms, morning report and daily morning holdover emails. At the end of this trial, survey data showed that the majority of framework components were rated important and facilitated transfer. However, broader implementation revealed several barriers. Despite our dissemination, poor framework awareness among residents resulted in discrepancies in adoption. Also, framework interpretation varied as we lacked specific signout examples and role modeling. Finally, teams found it challenging to comply with the framework when computers were not readily available.
Conclusions:
Our pilot suggests that a standardized framework for holdover signout may improve signout efficiency and educational value. However, broad implementation of the framework necessitates continued work to improve framework awareness, delineate provider roles, and acquire appropriate resources to support expansion. Further work will focus on reducing these barriers and investigating the effect of the holdover framework on the safety of holdover signout.