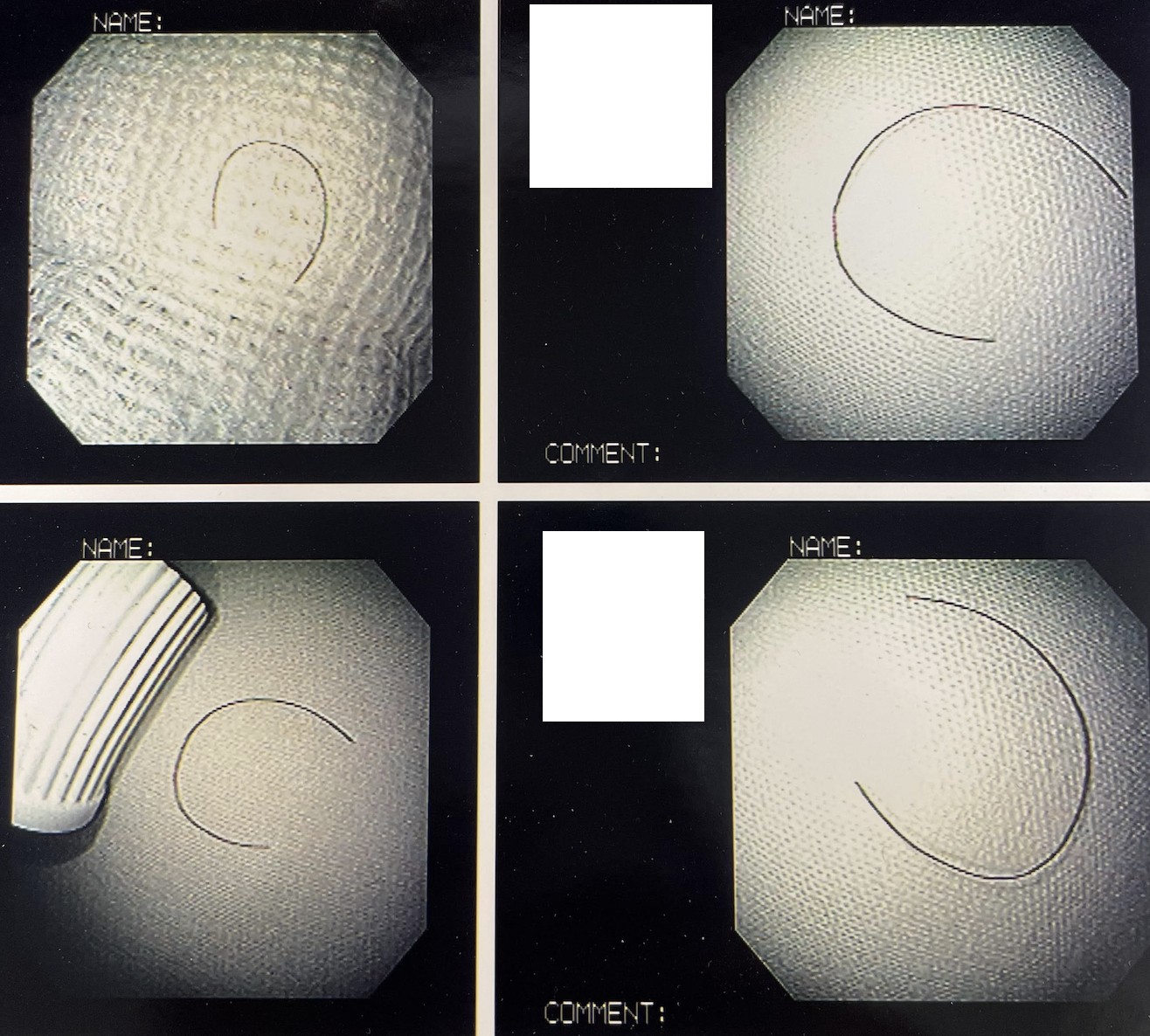
Case Presentation: A 53-year-old Asian female with no significant past medical history and a lifelong non-smoker without any chronic secondhand smoke exposure presented with a long-standing chronic non-productive cough that persisted over many years. The patient was not taking any prescribed medication(s) or over the counter supplements. Review of symptoms was negative for fever, chills, shortness of breath, rhinorrhea, sinus congestion, postnasal drip, dental or gum pain or heartburn. Previous work up consisting of chest x-ray, computerized tomography, pulmonary function tests, and upper GI series were all negative. A flexible fiberoptic bronchoscopy performed offered no answers, and the cough persisted. On the brink of giving up due to persistent symptoms without relief or answers, the patient was referred to a second pulmonologist for consultation. It was during this visit that a thorough examination of the patient’s ears, nose and throat was performed. Inspection of the left auditory canal yielded evidence of a foreign object, described as a hair-like projection. In conjunction with ENT consultation, visual analysis and retrieval yielded a 0.5 cm long hair. Upon removal, the patient broke down into tears after immediate relief and complete resolution of her cough.
Discussion: The complexity of cough, an innate primitive reflex aimed to protect the airway against irritants, has perplexed many astute clinicians with its wide array of presentations. It is regarded as one of the most common reasons a patient may seek care in the outpatient setting, leading to approximately 30 million clinical encounters per year in the United States alone [1]. While the most common causes of chronic cough are upper airway cough syndrome (UACS), asthma, non-asthmatic eosinophilic bronchitis (NAEB), COPD and gastroesophageal reflux disease (GERD), uncommon causes encompassing roughly 13.1% pose a greater struggle to the population at large [2]. Amongst these, Arnold’s reflex, first described by Friedrich Arnold in 1832, has gained increasing recognition as another possible uncommon cause of cough owing to increased hypersensitivity of vagal afferent nerves.
Conclusions: Often leading to misdiagnosis with inappropriate treatment for an unspecified time frame, uncommon causes of common conditions further negatively impact overall quality of life and worsen economic burdens. As Arnold’s nerve arises from the superior ganglion of the vagus nerve within the jugular foramen and innervates portions of the ear, any inducement of this reflex from irritation and basic mechanical stimulation including impacted foreign bodies, cerumen, and rarely hair involves the integration of both ongoing airway vagal afferent nerve input with additional input arising from the ear [3]. While this reflex has only been noted in a small fraction of patients in the past, a recent study found a higher prevalence of Arnold’s nerve reflex sensitivity in patients with chronic cough compared to healthy individuals [4]. Our case emphasizes the significance of a stepwise approach, thorough history and important historical aspects include smoking status, current medications, and concurrent symptoms. Understanding the mechanism of cough, its potential causes, performing a systematic and comprehensive physical exam which should include an otoscopic evaluation are essential in identifying the etiology and treatment for this common patient complaint.