Background: Disparities in health outcomes that differ by racial or ethnic group, religion, socioeconomic status, gender, age, mental health, ability, sexual orientation or gender identity, geographic location, or other characteristics historically linked to discrimination or exclusion demonstrate that equitable care in the United States is a goal that has not been achieved. Treating all patients equally does not eliminate health disparities; providers ignoring their own cultural background and biases when delivering health care to patients does not eliminate health disparities; equal access to health care does not eliminate health disparities; these and other misconceptions exist among health care providers. We developed an innovative curriculum conducted over a half-day seminar to new and seasoned physicians in order to test and break those misconceptions. Physicians have a choice to attend half-day workshops for faculty development and all participants had volunteered to attend this seminar.
Purpose: To teach a curriculum that serves to break misconceptions about health disparities and provide tools for practicing equitable care.
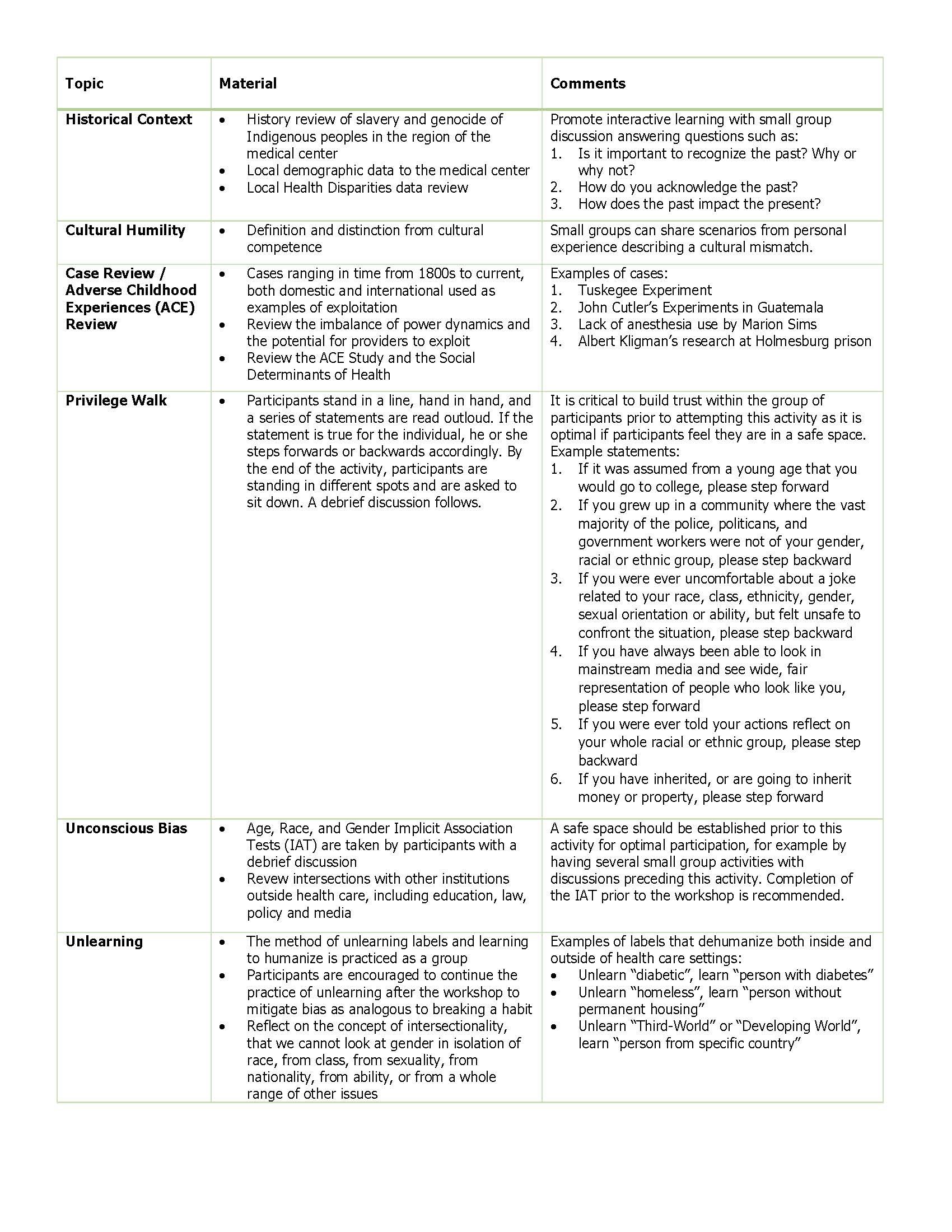
Description: Description: It is inadequate to discuss poverty without oppression, race without racism, income inequality without capitalism, gender inequality without sexism… Avoidance of the roots contributing to inequity in health care presents to the learner a redacted curriculum that will always lead to a perpetuation of inequity, only with the new guise of awareness. This curriculum about health equity and disparities is presented in 5-hours in an interactive style including polling, small group discussions, case reviews and presentations, and debriefing activities. The curriculum content is presented in Table 1.
Post-intervention survey showed participants ranking their understanding of health disparities from average/good to good/great. True/False statements were used to demonstrate misconceptions, for example, “the Tuskegee experiments were conducted to treat adult African Americans suffering from syphilis” showed 66.7% correct pre-seminar compared to 100% post-seminar. Confidence was also measured after each statement and for the example given, confidence increased from 4.2 to 4.9 on a 5-point scale.
Conclusions: Including the historical and political roots of inequity in a curriculum is necessary if the perpetuation of health disparities is to end. Presentation of the topics of this curriculum resulted in participants gaining confidence in their ability to address health care disparities. The tool of unlearning provides participants with a plan for mitigating against their unconscious bias. The road to health equity is long, and this novel curriculum is but a small step forward.