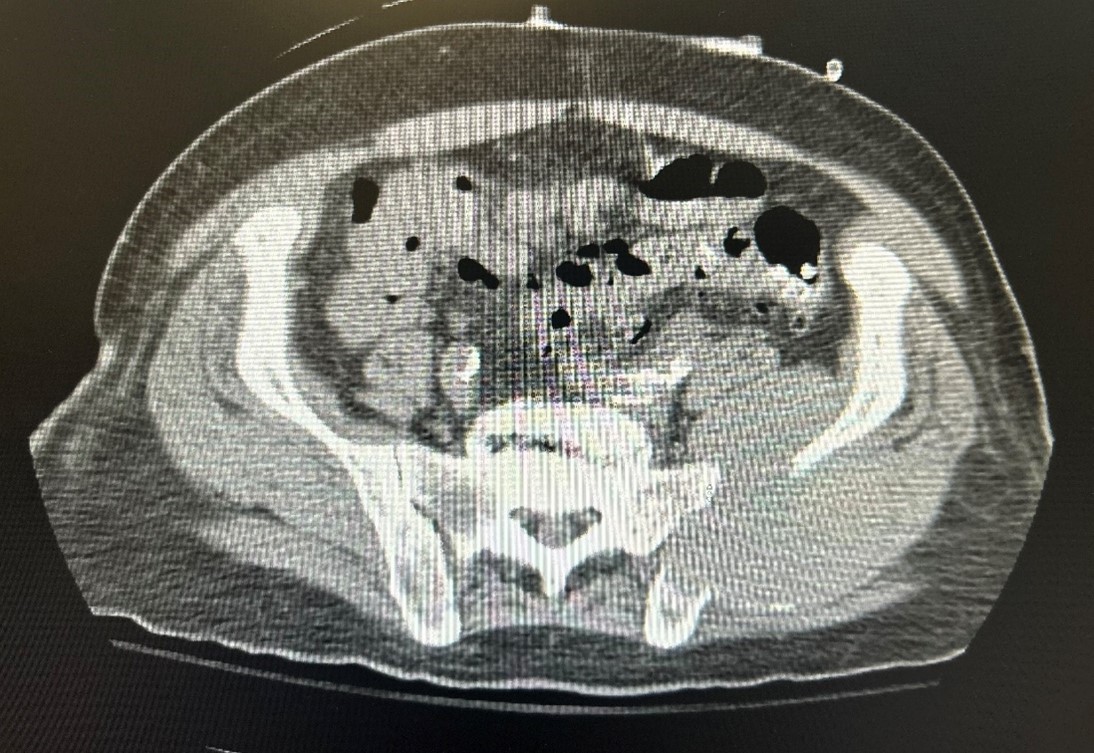
Case Presentation: A 70-year-old male with a history of hypertension, hyperlipidemia, cerebrovascular accident (CVA), benign prostatic hyperplasia (BPH), anemia, atrial fibrillation (AFib), coronary artery disease (CAD), and gastroesophageal reflux disease (GERD) presented with gross hematuria and abdominal pain. He had recently been discharged after treatment for a subdural hematoma and had a long-term Foley catheter placed due to subdural hematoma, removed the day before this admission. The patient was also being treated for a Pseudomonas-positive urinary tract infection (UTI) from a prior hospitalization. On presentation of this admission, he denied chest pain, shortness of breath, fever, or chills but reported abdominal pain and dysuria. Urology was consulted, and continuous bladder irrigation (CBI) was initiated. Initial CBC revealed anemia, Hgb 6.0, due to acute blood loss, and the patient was transfused with 4 units of packed red blood cells. Urinalysis showed a UTI with positive nitrates, leukocytes, and blood. Head CT confirmed a previous craniotomy with residual fluid in the subdural space. A bladder ultrasound suggested a diverticulum, and CT imaging revealed a fistula and two large masses, one near the bladder and another at the left iliac wing. The patient developed significant hematuria, requiring two additional blood transfusions. Initially, it was believed that these masses were sarcomas in nature. A CT-guided biopsy confirmed multiple myeloma, supported by electrophoresis. Given the complexity, the patient was transferred to a tertiary care facility for further management following a multidisciplinary conference.
Discussion: Although multiple myeloma is a malignancy that involved the bone marrow and can be suspected in patient based on preliminary blood work. This disorder can also initially be diagnosed when it involves other organs, as term coined extramedullary disease. Bladder involvement is particularly rare, with only a handful of cases reported. According to the most updated diagnostic criteria for multiple myeloma, in addition to the classic CRAB criteria (hypercalcemia, renal failure, anemia, and bone lesions), diagnosis now requires evidence of clonal plasma cell proliferation either in the bone marrow or as a solitary plasmacytoma. However, diagnosing solitary plasmacytoma necessitates the absence of clonal plasma cells in the bone marrow, normal imaging studies, and no signs of end-organ damage.This patient presented with atypical features, including anemia due to acute blood loss, the absence of hypercalcemia and back pain, but with evidence of metastatic bone lesions. Further investigation through biopsy confirmed the diagnosis of atypical systemic multiple myeloma.
Conclusions: While atypical presentations of multiple myeloma are known, hematuria associated with a bladder mass and fistula is an uncommon manifestation. A comprehensive evaluation is crucial for diagnosing such unusual presentations, as these rare symptoms can easily be mistaken for other conditions. Considering a broad differential diagnosis ensures accurate identification of the underlying cause and facilitates appropriate treatment.