Background: Hospitalizations related to opioid use disorder (OUD) are rising, creating opportunities to initiate medications for opioid use disorder (MOUD) and connect patients with outpatient resources.1,2 Despite evidence that MOUD reduces morbidity and mortality, most patients fail to receive evidence-based treatment during hospitalization.3-6 Addiction consultation services are becoming the standard of care to address this gap, but they are not available at all institutions.7-9 Thus, alternative strategies are needed to optimize inpatient MOUD access.
Purpose: We piloted a volunteer hospitalist-led MOUD team within our academic hospitalist group. The primary goal was to increase MOUD initiation in the inpatient setting, with a secondary aim to link patients to outpatient addiction services after discharge. This project was inspired by the buprenorphine team started in Dell Seton Medical Center at The University of Texas at Austin in 2017.
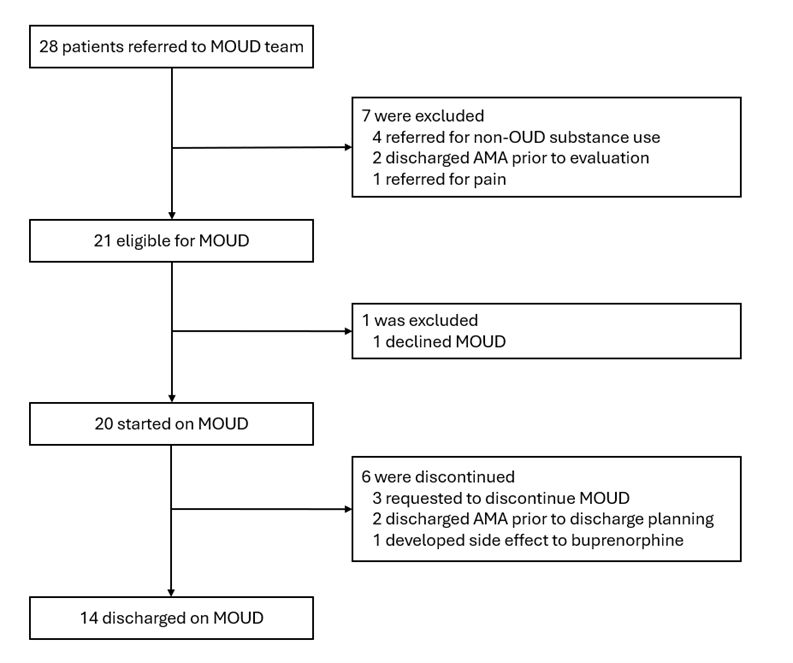
Description: The MOUD team was piloted over four months (July 2024-November 2024). Initially, the team was led by a single volunteer hospitalist and later expanded to include two more volunteer hospitalists.Baseline data was collected through hospital metrics and a hospitalist survey. Over the past three years, only 19% of eligible patients at our hospital were initiated on MOUD during hospitalization. Patients not started on MOUD had higher rates of 30-day hospital readmission (41% vs 21%), 30-day ED visits (28% vs 25%), length of stay (9.9 days vs 9.4 days), and patient-directed discharge (12% vs 8%).Our survey showed most hospitalists feel comfortable managing withdrawal but lack confidence in initiating and managing MOUD (Fig. 1). They also expressed a need for more consultant support and highlighted the ineffectiveness of the current post-discharge linkage process.We used a secure hospital messaging platform to encourage hospitalists to identify MOUD candidates and notify the MOUD team. The MOUD team evaluated these patients and determined eligibility based on two criteria: (1) meeting DSM-5 criteria for OUD, and (2) expressing a desire to reduce or stop opioid use.During the four-month pilot, 28 patients were referred to the MOUD team, with 21 meeting eligibility for MOUD initiation (Fig. 2). Of the eligible patients, 20 (95%) were started on MOUD during their hospitalization, and 14 (67%) were discharged on MOUD. All 14 patients were referred for outpatient follow-up. Notably, no MOUD recipients were readmitted to the ED or hospital within 30 days of discharge.
Conclusions: Volunteer, hospitalist-led MOUD teams can help fill the gap in initiating MOUD and connecting patients to outpatient addiction resources. Early results suggest MOUD initiation may also reduce healthcare utilization, including hospital readmissions.