
Background:
Vancomycin is commonly used in an empiric antimicrobial regimen. The joint 2009 AHSP/IDSA/SIDP guidelines recommend a minimum trough of 10 μg/mL to avoid development of rcsistance and troughs up to 20 μg/mL to improve tissue penetration and for complicated infections. We had previously discovered that vancomycin dosing practices at our institution resulted in 34% of initial troughs less than 10 μg/mL and only 51% in the 10‐20 μg/mL therapeutic range, with significant implications for efficacy of antimicrobial therapy in the crucial first days of illness, A multidisciplinary intervention was therefore implemented to improve the initial dosing.
Methods:
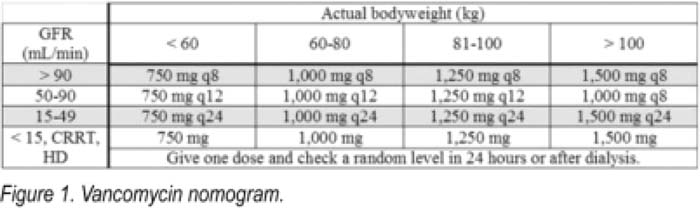
Consecutive medical intensive care unit patients at a tertiary academic center were included as long as they had a vancomycin trough checked. Baseline data were collected in June–August 2008, with postintervention data from August to November 2009. Using the best available evidence, a nomogram was created to determine the initial vancomycin dose (Fig. 1). The nomogram utilized actual body weight and glomerular filtration rate (GFR) estimated with the MDRD4 equation. The dose was based on the 2009 guidelines, which recommend 15–20 mg/kg every 8–2 hours, The prescribing providers were instructed to order “vancomycin per pharmacy,” with the clinical pharmacist determining the dose with the aid of a nomogram.
Results:
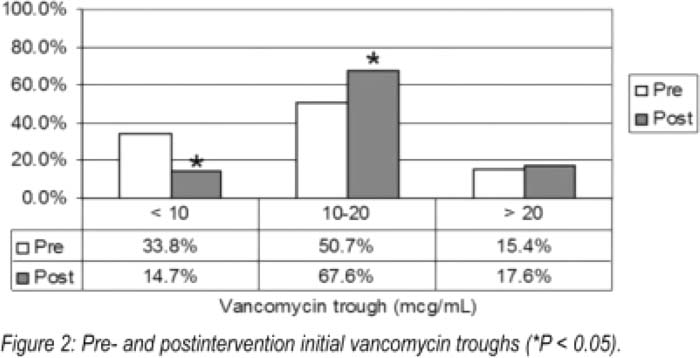
The preintervention (n = 65) and postintervention (n = 68) cohorts had similar demographics, with, respectively, an average age of 53.8 and 51.5 years, 46% and 50% female, 84.1 and 88.4 kg actual body weight, and 87.4 and 86.3 mL/min/1.73 m2 estimated GFR. The average total daily vancomycin dose was similar among pre‐ and postintervention groups (2211 vs. 2221 mg, P = 0.67), and there was no significant difference in average troughs (14.5 vs. 16.3 μg/mL, P = 0.24). Following the intervention, the proportion of troughs less than 10 μg/mL significantly decreased (33.8%‐14.7%, 1‐tailed P = 0.008), whereas the proportion of troughs in the 10‐20 μg/mL therapeutic range significantly increased (50.7% vs. 67.6%, 1‐tailed P = 0.035; Fig. 2). There was no difference in the proportion of troughs more than 20 μg/mL (15.4% vs. 17.6%, P = 0.81). An improvement in therapeutic troughs of similar magnitude was also seen in subgroups, including patients with GFR < 60 or > 90 and patients at the extremes of body weight (< 60 or > 100 kg).
Conclusions:
A multidisciplinary intervention utilizing pharmacist‐guided and nomogram‐based dosing significantly improves the proportion of therapeutic initial vancomycin troughs and decreases the number of subtherapeutic troughs by half.
Author Disclosure:
D. Levin, none; T. Kiser, none.