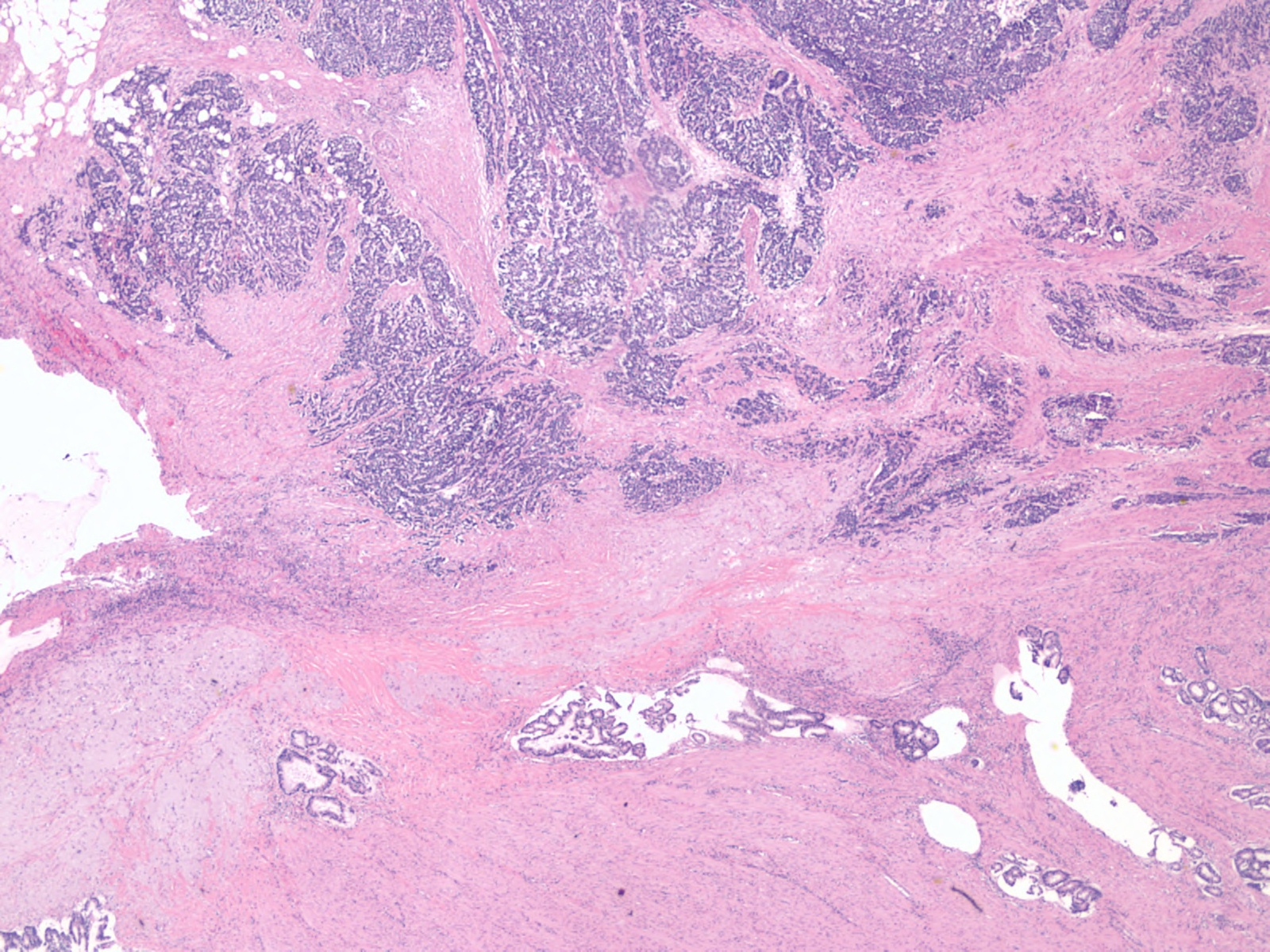
Case Presentation: A 71-year-old man with a history of Meckel’s diverticulum diagnosed by CT scan 10 months prior, diverticulitis, colonic polyps, intestinal hernias, iron deficiency anemia, and hypothyroidism presented to the ED with intermittent episodes of diffuse abdominal pain over the preceding 10 months with increasing frequency starting 3 days prior to arrival. Family history was significant for a sister with colon cancer diagnosed in her 30s. Routine colonoscopy 4 years prior revealed 13 polyps, which were removed. He had previously declined surgical intervention for his Meckel’s diverticulum, electing instead for conservative surveillance. Presenting vitals were stable, and labs were significant for his chronic anemia. CT abdomen demonstrated a partial small bowel obstruction within his known Meckel’s diverticulum. He was promptly taken to the OR for an uncomplicated exploratory laparotomy and ileal small bowel resection. Post-operative surgical pathology taken 15-20 cm from the ileocecal valve revealed high grade neuroendocrine carcinoma and moderately differentiated adenocarcinoma within the Meckel’s diverticulum that was also invasive to adjacent bowel. He was referred to oncology, and subsequently began chemotherapy.
Discussion: A neuroendocrine tumor (NET) is a rare and frequently asymptomatic neoplasm of neuroendocrine cells. Given the numerous primary site locations and the wide range of secretory granules produced by these cells, tumors often present obscurely, making symptomatic diagnosis challenging. NETs are most common in the gastrointestinal tract (41.8%) and the lungs (27.4%) due to the high density of neuroendocrine cells within these sites. NETs have been reported along the entire GI tract from esophagus to anus although most commonly in the small intestine (29.0%) and rectum (27.4%). Symptoms vary considerably based on primary tumor location. Our patient’s tumor developed within his Meckel’s diverticulum, which has been reported in less than 200 cases. Although only 0.48% of NETs develop within a Meckel’s diverticulum, they are the most common neoplasm of a Meckel’s diverticulum. While the mechanism is unclear, some Meckel’s diverticuli contain a high density of parietal cells that is thought to provide an alkalotic environment favorable for NET development. The most common presentation of Meckel’s diverticulum NETs is obstruction, as seen with this patient. Although NETs are often thought to be relatively benign, 58.3% of small intestinal NETs are non-localized at diagnosis with a five-year survival of 60.5%. These indications do not solely represent benign tumors. The risk of lethal malignancy further emphasizes the importance of resecting a symptomatic Meckel’s diverticulum.
Conclusions: NETs can develop within a Meckel’s diverticulum, particularly those with an alkalotic environment. Given that small intestinal NETs are often non-localized at the time of diagnosis with a five-year survival of 60.5%, this case further emphasizes the importance of resecting a symptomatic Meckel’s diverticulum.