Background: High workloads in the inpatient setting affect clinician well-being, patient outcomes, and organizational performance, yet decisions around work-design rarely links to outcomes outside of productivity and financial measures. Emerging technologies, including EHR use data (i.e., clickstream data), may offer real-time insights into workload and work patterns when paired with clinician-, patient-, and organization-level outcomes. These tools may offer the opportunity to bring evidence to decision-making on work design as well as a more precise assessment of workload and its impact on care. We conducted a multi-site study linking clinician-reported workload, EHR-derived metadata, workforce outcomes, and patient outcomes.
Methods: We performed an observational study across 12 U.S. hospitals (June–Nov 2024). Data sources: clinician surveys (n = 420) assessing burnout, professional fulfillment, NASA Task Load Index, and intent to leave/reduce hours; EHR metadata (6 months of Epic Signal data aggregated weekly/monthly) including patients/day, time in system, and secure chat; patient outcomes (ICU transfers, LOS, mortality and other outcomes from the Vizient database). Predictors were identified using LASSO with cross-validation and knockoff filter for FDR control. Multivariable models estimated associations with burnout, fulfillment, intent to leave/reduce hours, ICU transfer, and LOS. Performance was evaluated using AUC, adjusted R², and Root Mean Squared Error (RMSE).
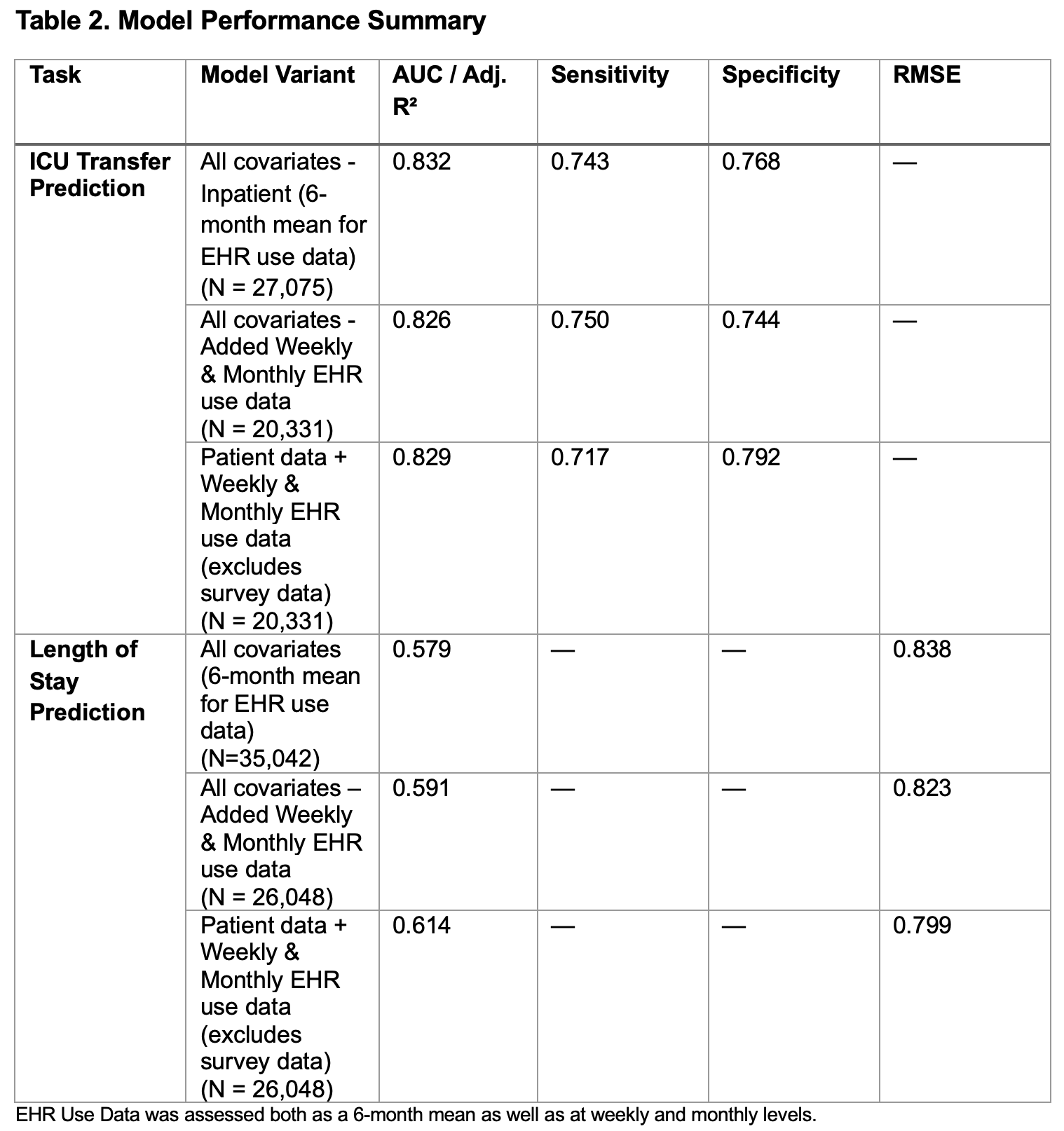
Results: Across 12 hospitals, 420 clinicians participated with 38,873 patients discharged by the participants. Burnout affected 50% of physicians and 61% of APPs; 71% of physicians and 56% of APPs had some intention to reduce clinical hours. Nearly three-fourths of participants did not meet professional fulfillment thresholds. EHR use data was moderately correlated with survey workload (patients/day r = 0.45, p < 0.0001) but underreported patient load (8 vs. 13/day). Integrated models combining EHR use data and survey data predicted burnout (AUC = 0.86) and intent to leave (AUC = 0.85); EHR use data-only models were moderate (AUC = 0.62–0.71). Fulfillment prediction was weaker (Adj. R² = 0.41).Linking EHR use data, surveys, and patient data showed work design associations with patient outcomes. ICU transfer models achieved AUC up to 0.83, sensitivity/specificity >0.74. LOS prediction using patient data plus weekly/monthly signals was strong (Adj. R² = 0.61); EHR-only explained less variance (Adj. R² = 0.13). Each additional patient/day was associated with an increased LOS by 5% (95% CI: 4% – 5%); more time in orders per patient/day increased LOS by 8% (95% CI: 7% – 9%). Higher order set use was associate with a lower LOS (~29% reduction; 95% CI: 24% – 34% reduction).
Conclusions: This study is among the first multi-hospital efforts to link work design with clinician, patient, and organizational-level outcomes using clinician surveys, EHR use data, and patient outcomes data. EHR use data showed moderate correlations with clinician-reported workloads; with EHR use measures associated with ICU transfer and length of stay. Together, these findings provide emerging evidence that work design measurably influences clinician experience and care delivery and offers a foundation for a precision-science, data-informed redesign effort moving forward.
.jpg)